国际口腔医学杂志 ›› 2021, Vol. 48 ›› Issue (5): 528-535.doi: 10.7518/gjkq.2021102
周万航1( ),李嫣斐2,许日聪3,万启军3()
),李嫣斐2,许日聪3,万启军3()
Zhou Wanhang1(),Li Yanfei2,Xu Ricong3,Wan Qijun3()
摘要:
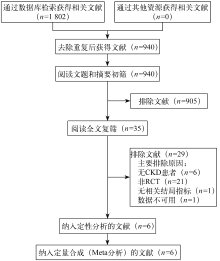
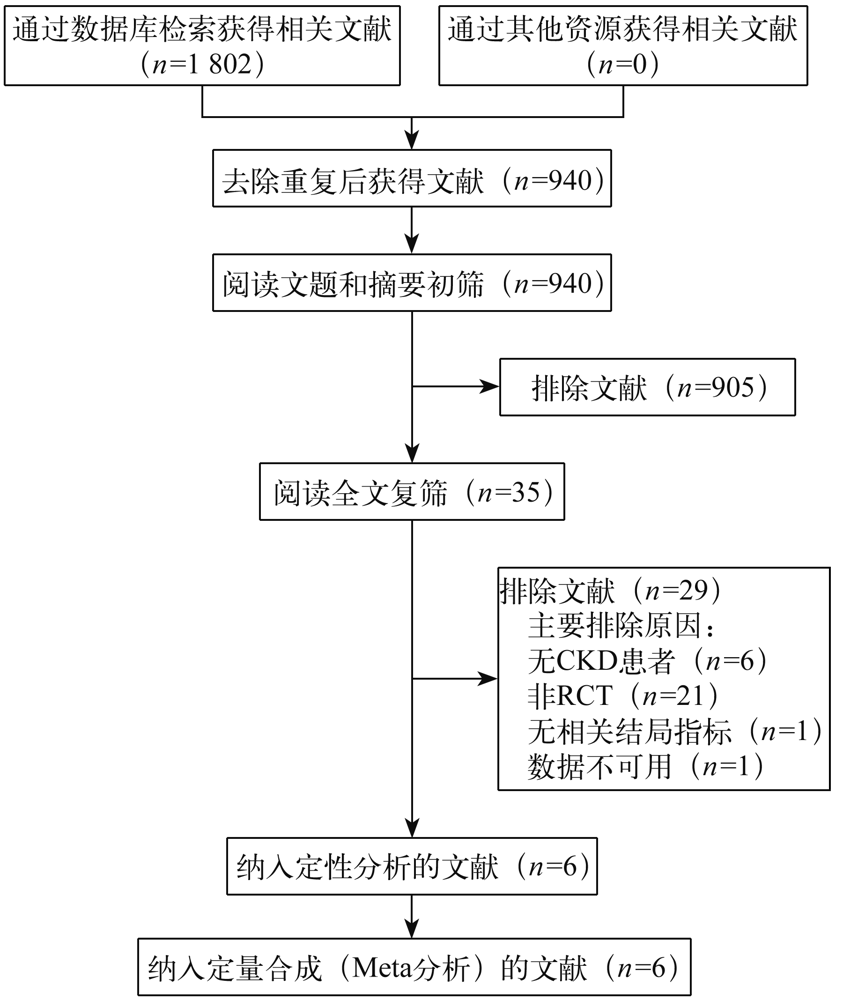
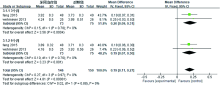
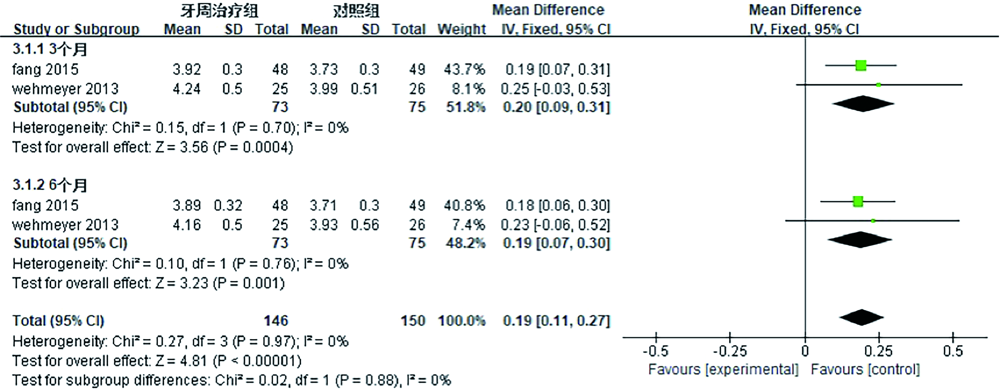
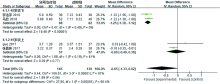
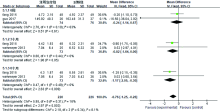
目的 系统评价牙周非手术治疗对慢性肾脏病(CKD)部分危险因素及全身炎症水平的影响,为CKD与牙周病的联合防治提供循证依据。方法 系统检索PubMed、Embase、Cochrane library、Science Direct、Scopus、Web of Science、CNKI、万方、维普中发表的相关文献,检索时间为从建库到2020年7月。由2名评价者独立筛选文献,评价文献质量,提取数据并评价纳入研究的偏倚风险后,采用RevMan 5.3软件进行Meta分析。结果 最终纳入6项随机对照试验(RCT),共432例患者。Meta分析结果显示:与无牙周干预的对照组相比,牙周非手术治疗能显著降低治疗前后CKD伴牙周病患者24 h尿蛋白定量分析水平[MD=-0.32,95%CI(-0.50,-0.14),P=0.000 4]、45岁以下患者血清C反应蛋白(CRP)[MD=-1.25,95%CI(-1.38,-1.12),P<0.000 01]及治疗后3、6个月白细胞介素-6(IL-6)水平[MD=-0.82,95%CI(-1.64,0.00),P=0.05;MD=-1.17,95%CI(-2.05,-0.30),P=0.009],并提高患者血清白蛋白(Alb)水平[MD=0.19,95%CI(0.11,0.27),P<0.000 01]。然而,对45岁以上患者血清CRP[MD=-0.06,95%CI(-0.48,0.36),P=0.77]及治疗后6周的血清IL-6[MD=-0.24,95%CI(-1.14,0.67),P=0.61]等,两组差异无统计学意义(P>0.05)。结论 牙周非手术治疗可降低CKD患者24 h尿蛋白定量分析水平,提高血清Alb水平,并可改善45岁以下患者的CRP和IL-6表达状况。
中图分类号:
| [1] |
Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives[J]. Lancet, 2013, 382(9888):260-272.
doi: 10.1016/S0140-6736(13)60687-X |
| [2] | Chandy S, Joseph K, Sankaranarayanan A, et al. Evaluation of C-reactive protein and fibrinogen in patients with chronic and aggressive periodontitis: a clinico-biochemical study[J]. J Clin Diagn Res, 2017, 11(3): ZC41-ZC45. |
| [3] |
Sabharwal A, Gomes-Filho IS, Stellrecht E, et al. Role of periodontal therapy in management of common complex systemic diseases and conditions: an update[J]. Periodontol 2000, 2018, 78(1):212-226.
doi: 10.1111/prd.2018.78.issue-1 |
| [4] |
Kshirsagar AV, Moss KL, Elter JR, et al. Periodontal disease is associated with renal insufficiency in the Atherosclerosis Risk In Communities (ARIC) study[J]. Am J Kidney Dis, 2005, 45(4):650-657.
pmid: 15806467 |
| [5] | 周万航, 李嫣斐, 郭留云, 等. 牙周病与慢性肾病关系研究进展[J]. 中国实用口腔科杂志, 2019, 12(10):622-627. |
| Zhou WH, Li YF, Guo LY, et al. Research progress on the relationship between periodontal disease and chronic kidney disease[J]. Chin J Pract Stomatol, 2019, 12(10):622-627. | |
| [6] |
Sharma P, Dietrich T, Sidhu A, et al. The periodontal health component of the Renal Impairment In Secondary Care (RIISC) cohort study: a description of the rationale, methodology and initial baseline results[J]. J Clin Periodontol, 2014, 41(7):653-661.
doi: 10.1111/jcpe.12263 |
| [7] |
Oyetola EO, Owotade FJ, Agbelusi GA, et al. Oral findings in chronic kidney disease: implications for management in developing countries[J]. BMC Oral Health, 2015, 15:24.
doi: 10.1186/s12903-015-0004-z pmid: 25888327 |
| [8] |
Ricardo AC, Athavale A, Chen JS, et al. Periodontal disease, chronic kidney disease and mortality: results from the third National Health and Nutrition Examination Survey[J]. BMC Nephrol, 2015, 16:97.
doi: 10.1186/s12882-015-0101-x pmid: 26149680 |
| [9] |
Grubbs V, Vittinghoff E, Beck JD, et al. Association between periodontal disease and kidney function decline in African Americans: the Jackson heart study[J]. J Periodontol, 2015, 86(10):1126-1132.
doi: 10.1902/jop.2015.150195 |
| [10] |
Sharma P, Dietrich T, Ferro CJ, et al. Association between periodontitis and mortality in stages 3-5 chro-nic kidney disease: NHANESⅢand linked mortality study[J]. J Clin Periodontol, 2016, 43(2):104-113.
doi: 10.1111/jcpe.2016.43.issue-2 |
| [11] |
Chambrone L, Foz AM, Guglielmetti MR, et al. Periodontitis and chronic kidney disease: a systema-tic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate[J]. J Clin Periodontol, 2013, 40(5):443-456.
doi: 10.1111/jcpe.12067 pmid: 23432795 |
| [12] |
Zhao D, Khawaja AT, Jin LJ, et al. Effect of non-surgical periodontal therapy on renal function in chro-nic kidney disease patients with periodontitis: a systematic review and Meta-analysis of interventional studies[J]. Clin Oral Investig, 2020, 24(4):1607-1618.
doi: 10.1007/s00784-019-03066-w |
| [13] |
Wehmeyer MM, Kshirsagar AV, Barros SP, et al. A randomized controlled trial of intensive periodontal therapy on metabolic and inflammatory markers in patients with ESRD: results of an exploratory study[J]. Am J Kidney Dis, 2013, 61(3):450-458.
doi: 10.1053/j.ajkd.2012.10.021 pmid: 23261122 |
| [14] | Guo N, Lin G. Effects of nonsurgical periodontal therapy on serum inflammatory factor levels in patients with chronic kidney disease and periodontitis[J]. Biomed Res, 2017, 28(9):3899-3902. |
| [15] | Fang FC, Wu BL, Qu Q, et al. The clinical response and systemic effects of non-surgical periodontal the-rapy in end-stage renal disease patients: a 6-month randomized controlled clinical trial[J]. J Clin Perio-dontol, 2015, 42(6):537-546. |
| [16] | 李浩萍, 李明勇. 慢性肾病伴牙周炎患者牙周基础治疗疗效及对肾功能指标的影响[J]. 北华大学学报(自然科学版), 2018, 19(3):374-377. |
| Li HP, Li MY. Therapeutic effect of periodontal ba-sic treatment in patients with chronic renal disease and periodontitis and its effect on renal function[J]. J Beihua Univ Nat Sci, 2018, 19(3):374-377. | |
| [17] | 马欣, 李昊, 丑海燕, 等. 牙周基础治疗对慢性肾脏病伴牙周炎患者牙周指数及龈沟液炎性因子和肾功能指标的影响[J]. 中华实用诊断与治疗杂志, 2018, 32(3):255-257. |
| Ma X, Li H, Chou HY, et al. Effect of periodontal therapy on periodontal index, gingival crevicular fluid inflammatory factors and renal indexes in patients with chronic kidney disease and periodontitis[J]. J Chin Pract Diagn Ther, 2018, 32(3):255-257. | |
| [18] | 张晋玮, 刘建山, 马明, 等. 牙周基础治疗对行腹膜透析牙周炎患者的影响[J]. 天津医药, 2017, 45(3):282-284. |
| Zhang JW, Liu JS, Ma M, et al. Effects of periodon-tal basic treatment on peritoneal dialysis in patients with periodontitis[J]. Tianjin Med J, 2017, 45(3):282-284. | |
| [19] |
Stevens PE, Levin A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline[J]. Ann Intern Med, 2013, 158(11):825-830.
doi: 10.7326/0003-4819-158-11-201306040-00007 pmid: 23732715 |
| [20] | Cholewa M, Madziarska K, Radwan-Oczko M. The association between periodontal conditions, inflammation, nutritional status and calcium-phosphate metabolism disorders in hemodialysis patients[J]. J Appl Oral Sci, 2018, 26:e20170495. |
| [21] |
Lim CC, Teo BW, Ong PG, et al. Chronic kidney disease, cardiovascular disease and mortality: a prospective cohort study in a multi-ethnic Asian population[J]. Eur J Prev Cardiol, 2015, 22(8):1018-1026.
doi: 10.1177/2047487314536873 |
| [22] | Melsom T, Solbu MD, Schei J, et al. Mild albumi-nuria is a risk factor for faster GFR decline in the nondiabetic population[J]. Kidney Int Rep, 2018, 3(4):817-824. |
| [23] |
Lambers Heerspink HJ, Gansevoort RT. Albumi-nuria is an appropriate therapeutic target in patients with CKD: the proview[J]. Clin J Am Soc Nephrol, 2015, 10(6):1079-1088.
doi: 10.2215/CJN.11511114 |
| [24] |
Kubo S, Kitamura A, Imano H, et al. Serum albumin and high-sensitivity C-reactive protein are independent risk factors of chronic kidney disease in middle-aged Japanese individuals: the circulatory risk in communities study[J]. J Atheroscler Thromb, 2016, 23(9):1089-1098.
doi: 10.5551/jat.33530 |
| [25] |
Walther CP, Gutiérrez OM, Cushman M, et al. Serum albumin concentration and risk of end-stage renal disease: the REGARDS study[J]. Nephrol Dial Transplant, 2018, 33(10):1770-1777.
doi: 10.1093/ndt/gfx331 |
| [26] | Cohen SA, Kopp RP, Palazzi KL, et al. Association of rise in C-reactive protein with decline in renal function following partial nephrectomy[J]. Can J U-rol, 2015, 22(6):8085-8092. |
| [27] |
Kugler E, Cohen E, Goldberg E, et al. C reactive protein and long-term risk for chronic kidney disease: a historical prospective study[J]. J Nephrol, 2015, 28(3):321-327.
doi: 10.1007/s40620-014-0116-6 pmid: 24981713 |
| [28] |
Li WJ, Chen XM, Nie XY, et al. Cardiac troponin and C-reactive protein for predicting all-cause and cardiovascular mortality in patients with chronic kidney disease: a meta-analysis[J]. Clinics (Sao Paulo), 2015, 70(4):301-311.
doi: 10.6061/clinics |
| [29] | Santos-Paul MA, Neves RS, Gowdak LHW, et al. Cardiovascular risk reduction with periodontal treatment in patients on the waiting list for renal transplantation[J]. Clin Transplant, 2019, 33(8):e13658. |
| [30] | Huang ST, Yu TM, Ke TY, et al. Intensive periodontal treatment reduces risks of hospitalization for cardiovascular disease and all-cause mortality in the hemodialysis population[J]. J Clin Med, 2018, 7(10):E344. |
| [1] | 古丽其合热·阿布来提,秦旭,朱光勋. 线粒体自噬在牙周炎发生发展过程中的研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 68-73. |
| [2] | 龚佳明,赵瑞敏,潘宏伟,郎鑫,余占海,李健学. 动态导航与静态导航对种植体准确性的Meta分析[J]. 国际口腔医学杂志, 2023, 50(5): 538-551. |
| [3] | 李转转,格根塔娜. 牙髓血运重建术和根尖诱导成形术疗效对比的Meta分析[J]. 国际口腔医学杂志, 2023, 50(2): 177-185. |
| [4] | 成益凡,秦旭,姜鸣,朱光勋. 牙周病中固有淋巴细胞的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 32-36. |
| [5] | 李伟光,吴亚菲,郭淑娟. 无机纳米粒子在牙周病诊疗中的研究进展[J]. 国际口腔医学杂志, 2022, 49(6): 724-730. |
| [6] | 龚佳明,赵瑞敏,李婉昕,苏琳涵,余占海,李健学. 根盾技术对即刻种植临床效果的影响:基于随机对照研究的Meta分析[J]. 国际口腔医学杂志, 2022, 49(5): 537-547. |
| [7] | 张珊,葛晓磊,李杰,谢新宇,常维维,马文盛. 上颌前方牵引矫治对颌骨生长发育长期影响的Meta分析[J]. 国际口腔医学杂志, 2022, 49(5): 548-555. |
| [8] | 马玉,左玉,张鑫. 光动力疗法辅助治疗牙周炎治疗效果的Meta分析[J]. 国际口腔医学杂志, 2022, 49(3): 305-316. |
| [9] | 李归平,秦旭,朱光勋. 腺苷酸活化蛋白激酶在牙周病发生发展中的研究进展[J]. 国际口腔医学杂志, 2022, 49(3): 343-348. |
| [10] | 郭子源,常笑,韩开放,张锡忠. 低能量激光促进正畸牙移动有效性研究的系统评价与Meta分析[J]. 国际口腔医学杂志, 2022, 49(2): 163-172. |
| [11] | 穆新月,刘树泰. 动机性访谈在牙周病患者临床管理中的应用进展[J]. 国际口腔医学杂志, 2022, 49(1): 94-99. |
| [12] | 黄晓慧,祁本婷,杨洁,刘玉,孙卫斌. 机械性邻面菌斑控制措施对牙周非手术治疗效果影响的系统评价[J]. 国际口腔医学杂志, 2021, 48(6): 656-663. |
| [13] | 白皓亮,杨禾,赵蕾. 牙周病风险评估及预后判断工具的研究进展[J]. 国际口腔医学杂志, 2021, 48(6): 696-702. |
| [14] | 沈忆芬,刘超,汤颖,顾永春. 电子烟暴露对牙周健康影响的研究进展[J]. 国际口腔医学杂志, 2021, 48(3): 347-353. |
| [15] | 秦小茹,刘梦圆. 牙周病和心肌梗死发生风险相关性队列研究的Meta分析[J]. 国际口腔医学杂志, 2021, 48(2): 165-172. |
|