国际口腔医学杂志 ›› 2019, Vol. 46 ›› Issue (2): 125-134.doi: 10.7518/gjkq.2019001
• 专家笔谈 • 下一篇
郭淑娟,刘倩,丁一( )
)
Shujuan Guo,Qian Liu,Yi Ding()
摘要:
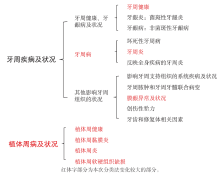
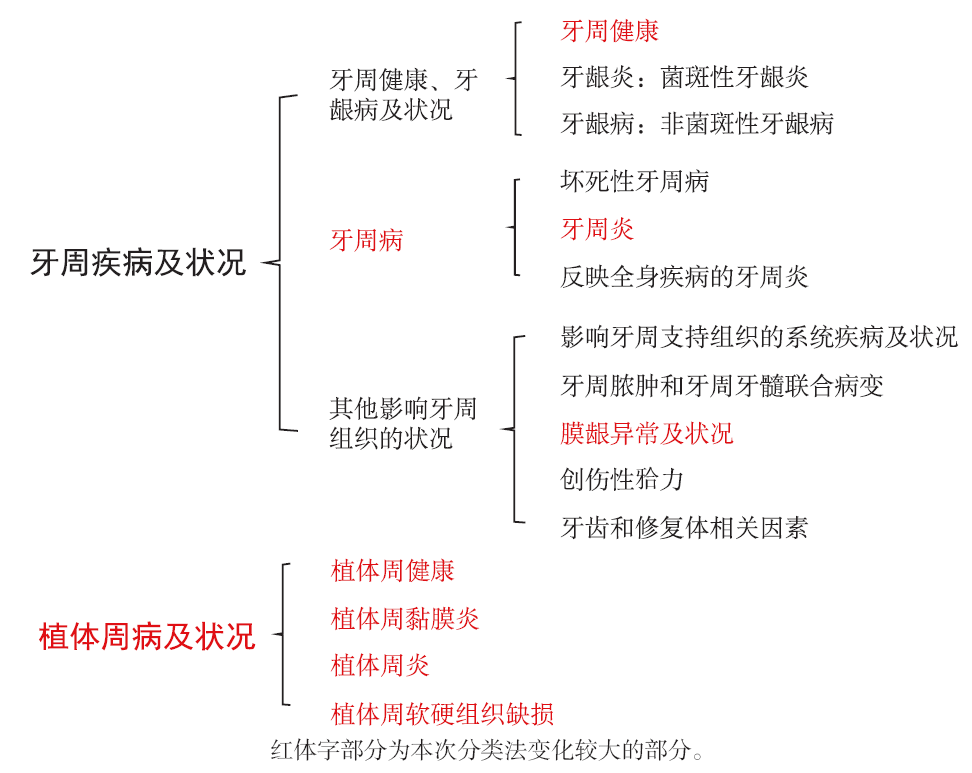
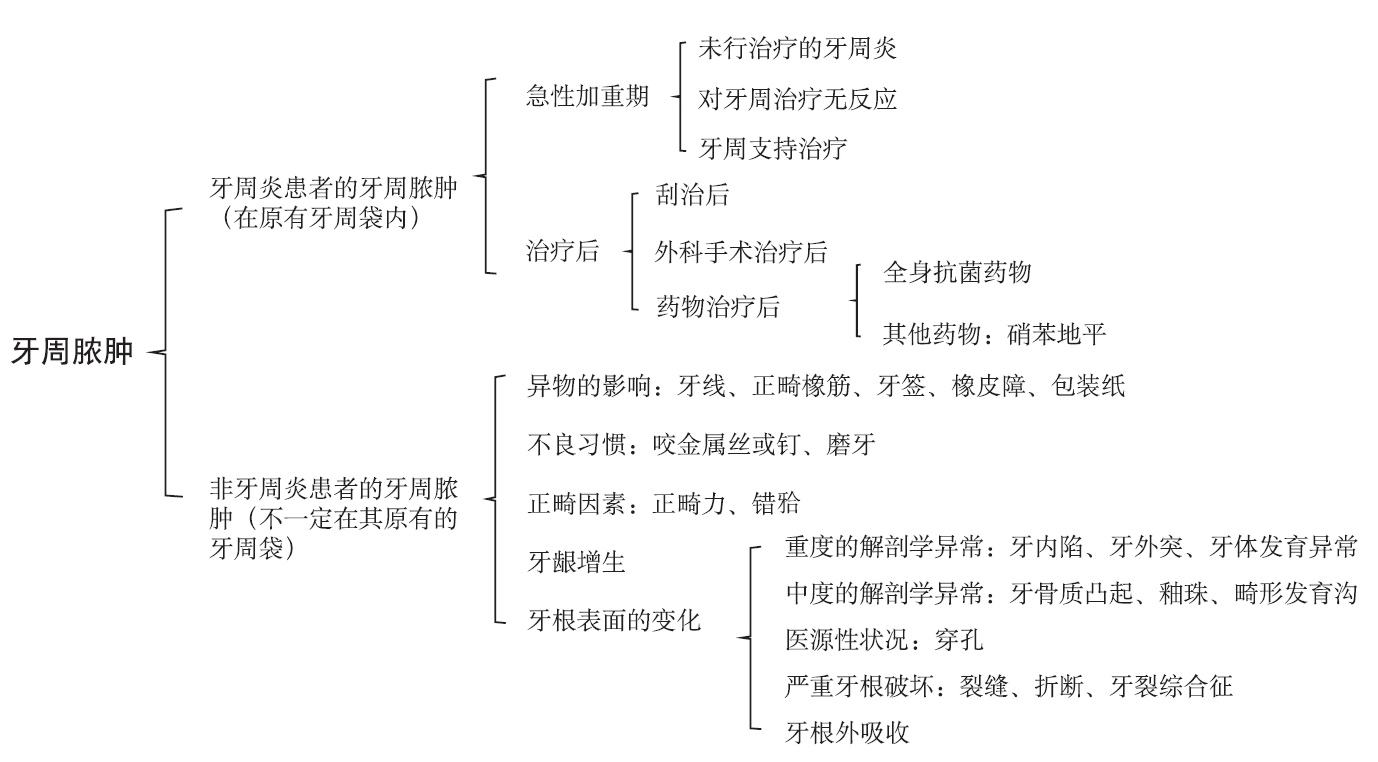
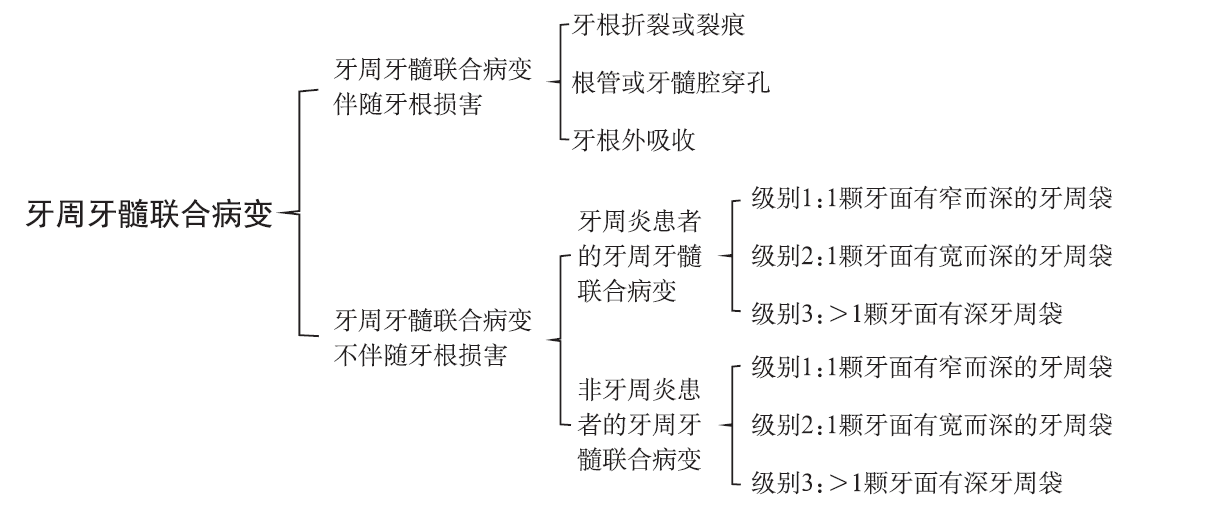
2018年欧洲牙周病联合会(EFP)与美国牙周病学会(AAP)组织召开了牙周病和植体周病新分类国际研讨会,经会议讨论后形成了一致的共识性报告,本文将对该报告的主要内容进行简要介绍。
中图分类号:
| [1] |
Caton JG, Armitage G, Berglundh T , et al. A new classification scheme for periodontal and peri-implant diseases and conditions-introduction and key changes from the 1999 classification[J]. J Clin Periodontol, 2018,45(Suppl 20):S1-S8.
doi: 10.1002/JPER.18-0157 |
| [2] |
Chapple ILC, Mealey BL, Van Dyke TE , et al. Perio-dontal health and gingival diseases and conditions on an intact and a reduced periodontium: consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions[J]. J Clin Periodontol, 2018,45(Suppl 20):S68-S77.
doi: 10.1111/jcpe.12940 pmid: 29926499 |
| [3] |
Lang NP, Bartold PM . Periodontal health[J]. J Perio-dontol, 2018,89(Suppl 1):S9-S16.
doi: 10.1002/JPER.16-0517 |
| [4] |
Murakami S, Mealey BL, Mariotti A , et al. Dental plaque-induced gingival conditions[J]. J Periodontol, 2018,89(Suppl 1):S17-S27.
doi: 10.1002/JPER.17-0095 pmid: 29926503 |
| [5] |
Holmstrup P, Plemons J, Meyle J . Non-plaque-indu-ced gingival diseases[J]. J Clin Periodontol, 2018,45(Suppl 20):S28-S43.
doi: 10.1111/jcpe.12938 pmid: 29926497 |
| [6] |
Albandar JM, Susin C, Hughes FJ . Manifestations of systemic diseases and conditions that affect the perio- dontal attachment apparatus: case definitions and diagnostic considerations[J]. J Periodontol, 2018,89(Suppl 1):S183-S203.
doi: 10.1002/jper.16-0480 |
| [7] |
Jepsen S, Caton JG, Albandar JM , et al. Periodontal manifestations of systemic diseases and developmen-tal and acquired conditions: consensus report of work- group 3 of the 2017 World Workshop on the Classifi-cation of Periodontal and Peri-Implant Diseases and Conditions[J]. J Clin Periodontol, 2018,45(Suppl 20):S219-S229.
doi: 10.1002/JPER.17-0733 pmid: 29926943 |
| [8] | Wennström JL, Tomasi C, Bertelle A , et al. Full-mouth ultrasonic debridement versus quadrant scaling and root planing as an initial approach in the |
| treatment of chronic periodontitis [J]. J Clin Perio-dontol, 2005,32(8):851-859. | |
| [9] |
Trombelli L, Farina R, Silva CO , et al. Plaque-in-duced gingivitis: case definition and diagnostic con-siderations[J]. J Clin Periodontol, 2018,45(Suppl 20):S44-S67.
doi: 10.1002/JPER.17-0576 |
| [10] |
Ramseier CA, Mirra D, Schütz C , et al. Bleeding on probing as it relates to smoking status in patients enrolled in supportive periodontal therapy for at least 5 years[J]. J Clin Periodontol, 2015,42(2):150-159.
doi: 10.1111/jcpe.12344 pmid: 25469634 |
| [11] |
Papapanou PN, Sanz M, Buduneli N , et al. Periodon-titis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions[J]. J Perio- dontol, 2018,89(Suppl 1):S173-S182.
doi: 10.1002/JPER.17-0721 pmid: 29926951 |
| [12] |
Herrera D, Retamal-Valdes B, Alonso B , et al. Acute periodontal lesions (periodontal abscesses and necro-tizing periodontal diseases) and endo-periodontal lesions[J]. J Clin Periodontol, 2018,45(Suppl 20):S78-S94.
doi: 10.1111/jcpe.12941 |
| [13] |
Fan J, Caton JG . Occlusal trauma and excessive occ-lusal forces: narrative review, case definitions, and diagnostic considerations[J]. J Clin Periodontol, 2018,45(Suppl 20):S199-S206.
doi: 10.1111/jcpe.12949 |
| [14] |
Ercoli C, Caton JG . Dental prostheses and tooth-related factors[J]. J Clin Periodontol, 2018,45(Suppl 20):S207-S218.
doi: 10.1111/jcpe.12950 |
| [15] |
Simon JH, Glick DH, Frank AL . The relationship of endodontic-periodontic lesions[J]. J Periodontol, 1972,43(4):202-208.
doi: 10.1902/jop.1972.43.4.202 pmid: 1073910 |
| [16] |
Cortellini P, Bissada NF . Mucogingival conditions in the natural dentition: narrative review, case definitions, and diagnostic considerations[J]. J Clin Periodontol, 2018,45(Suppl 20):S190-S198.
doi: 10.1002/JPER.16-0671 pmid: 29926948 |
| [17] |
Zweers J, Thomas RZ, Slot DE , et al. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review[J]. J Clin Perio-dontol, 2014,41(10):958-971.
doi: 10.1111/jcpe.12275 pmid: 24836578 |
| [18] |
Cairo F, Nieri M, Cincinelli S , et al. The interpro-ximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study[J]. J Clin Periodon-tol, 2011,38(7):661-666.
doi: 10.1111/j.1600-051X.2011.01732.x pmid: 21507033 |
| [19] |
Berglundh T, Armitage G, Araujo MG , et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Disea-ses and Conditions[J]. J Clin Periodontol, 2018,45(Suppl 20):S286-S291.
doi: 10.1111/jcpe.2018.45.issue-S20 |
| [20] |
Renvert S, Persson GR, Pirih FQ , et al. Peri-implant health, peri-implant mucositis, and peri-implantitis: case definitions and diagnostic considerations[J]. J Clin Periodontol, 2018,45(Suppl 20):S278-S285.
doi: 10.1002/JPER.17-0588 |
| [21] |
Araujo MG, Lindhe J . Peri-implant health[J]. J Clin Periodontol, 2018,45(Suppl 20):S230-S236.
doi: 10.1111/jcpe.2018.45.issue-S20 |
| [22] |
Heitz-Mayfield LJA, Salvi GE . Peri-implant muco-sitis[J]. J Clin Periodontol, 2018,45(Suppl 20):S237-S245.
doi: 10.1111/jcpe.2018.45.issue-S20 |
| [23] |
Hämmerle CHF, Tarnow D . The etiology of hard- and soft-tissue deficiencies at dental implants: a narrative review[J]. J Clin Periodontol, 2018,45(Suppl 20):S267-S277.
doi: 10.1002/JPER.16-0810 pmid: 29926950 |
| [1] | 傅豫, 何薇, 黄兰. 铁死亡在口腔疾病中的研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 36-44. |
| [2] | 古丽其合热·阿布来提,秦旭,朱光勋. 线粒体自噬在牙周炎发生发展过程中的研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 68-73. |
| [3] | 罗晓洁,王德续,陈晓涛. 基于生物信息学分析铁死亡调控基因与牙周炎的关系[J]. 国际口腔医学杂志, 2023, 50(6): 661-668. |
| [4] | 黄元鸿,彭显,周学东. 骨碎补在治疗口腔骨相关疾病的研究进展[J]. 国际口腔医学杂志, 2023, 50(6): 679-685. |
| [5] | 龚美灵,程兴群,吴红崑. 牙周炎与帕金森病相关性的研究进展[J]. 国际口腔医学杂志, 2023, 50(5): 587-593. |
| [6] | 孙佳,韩烨,侯建霞. 白细胞介素-6-铁调素信号轴调控牙周炎相关性贫血致病机制的研究进展[J]. 国际口腔医学杂志, 2023, 50(3): 329-334. |
| [7] | 刘体倩,梁星,刘蔚晴,李晓虹,朱睿. 咬合创伤在牙周炎发生发展中的作用及机制的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 19-24. |
| [8] | 李琼,于维先. 白藜芦醇治疗牙周炎及其生物利用度的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 25-31. |
| [9] | 成益凡,秦旭,姜鸣,朱光勋. 牙周病中固有淋巴细胞的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 32-36. |
| [10] | 李伟光,吴亚菲,郭淑娟. 无机纳米粒子在牙周病诊疗中的研究进展[J]. 国际口腔医学杂志, 2022, 49(6): 724-730. |
| [11] | 黄伟琨,徐秋艳,周婷. 黄芩苷抑制脂多糖促巨噬细胞氧化应激损伤作用的研究[J]. 国际口腔医学杂志, 2022, 49(5): 521-528. |
| [12] | 周剑鹏,谢旭东,赵蕾,王骏. 辅助性T细胞17及白细胞介素17在牙周炎中的作用及机制的研究进展[J]. 国际口腔医学杂志, 2022, 49(5): 586-592. |
| [13] | 陈荟宇,白明茹,叶玲. 信号素3A与口腔常见病关系的研究进展[J]. 国际口腔医学杂志, 2022, 49(5): 593-599. |
| [14] | 周佳佳,赵蕾,徐欣. 牙周炎相关基因多态性的研究进展[J]. 国际口腔医学杂志, 2022, 49(4): 432-440. |
| [15] | 马玉,左玉,张鑫. 光动力疗法辅助治疗牙周炎治疗效果的Meta分析[J]. 国际口腔医学杂志, 2022, 49(3): 305-316. |
|