国际口腔医学杂志 ›› 2025, Vol. 52 ›› Issue (5): 634-643.doi: 10.7518/gjkq.2025095
陈玉1,2( ),雷银富3,吴和梅1,杜福兰4,党洁4,陈永梅1,陶明1(),石兴莲5
),雷银富3,吴和梅1,杜福兰4,党洁4,陈永梅1,陶明1(),石兴莲5
Yu Chen1,2(),Yinfu Lei3,Hemei Wu1,Fulan Du4,Jie Dang4,Yongmei Chen1,Ming Tao1(),Xinglian Shi5
摘要:
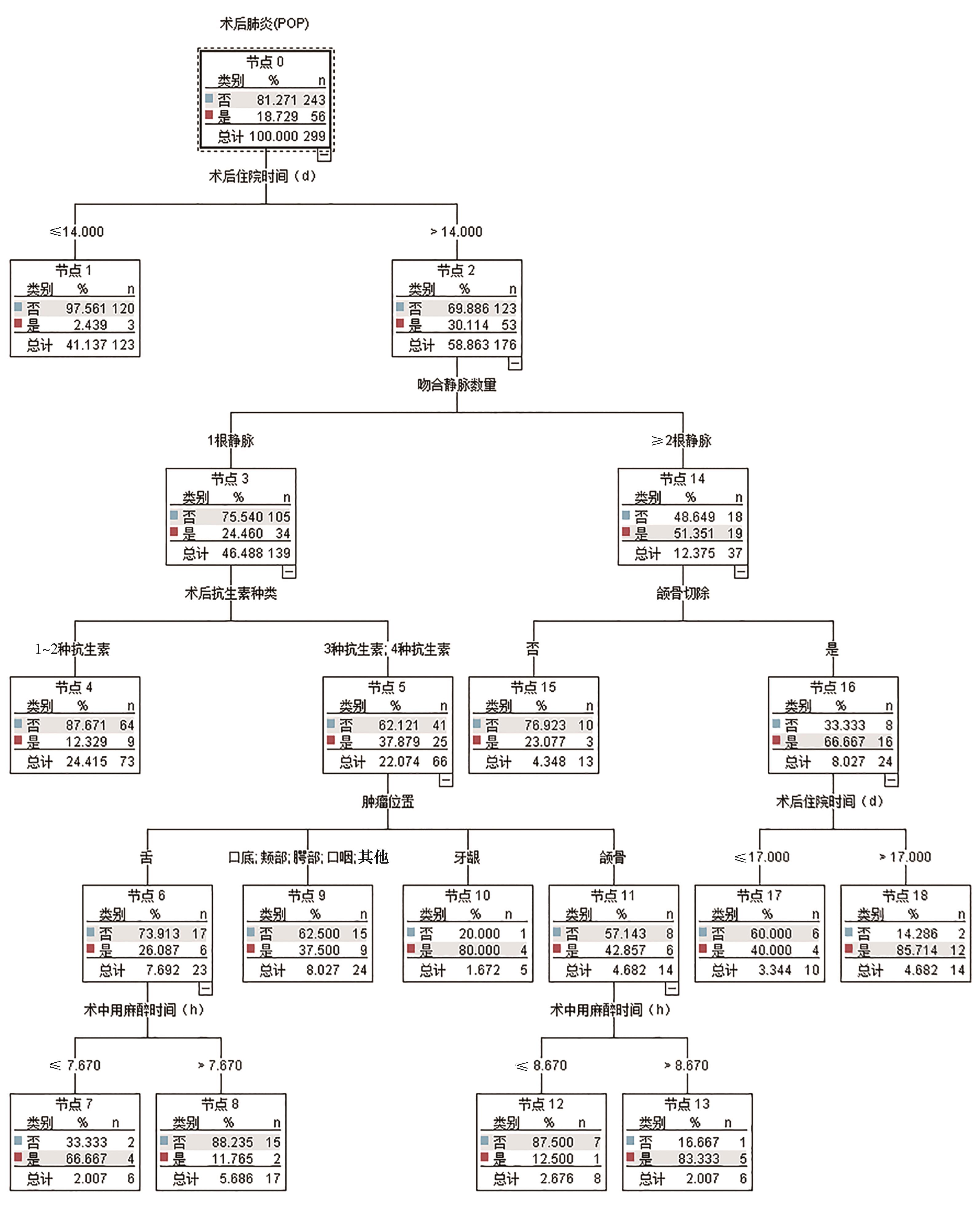
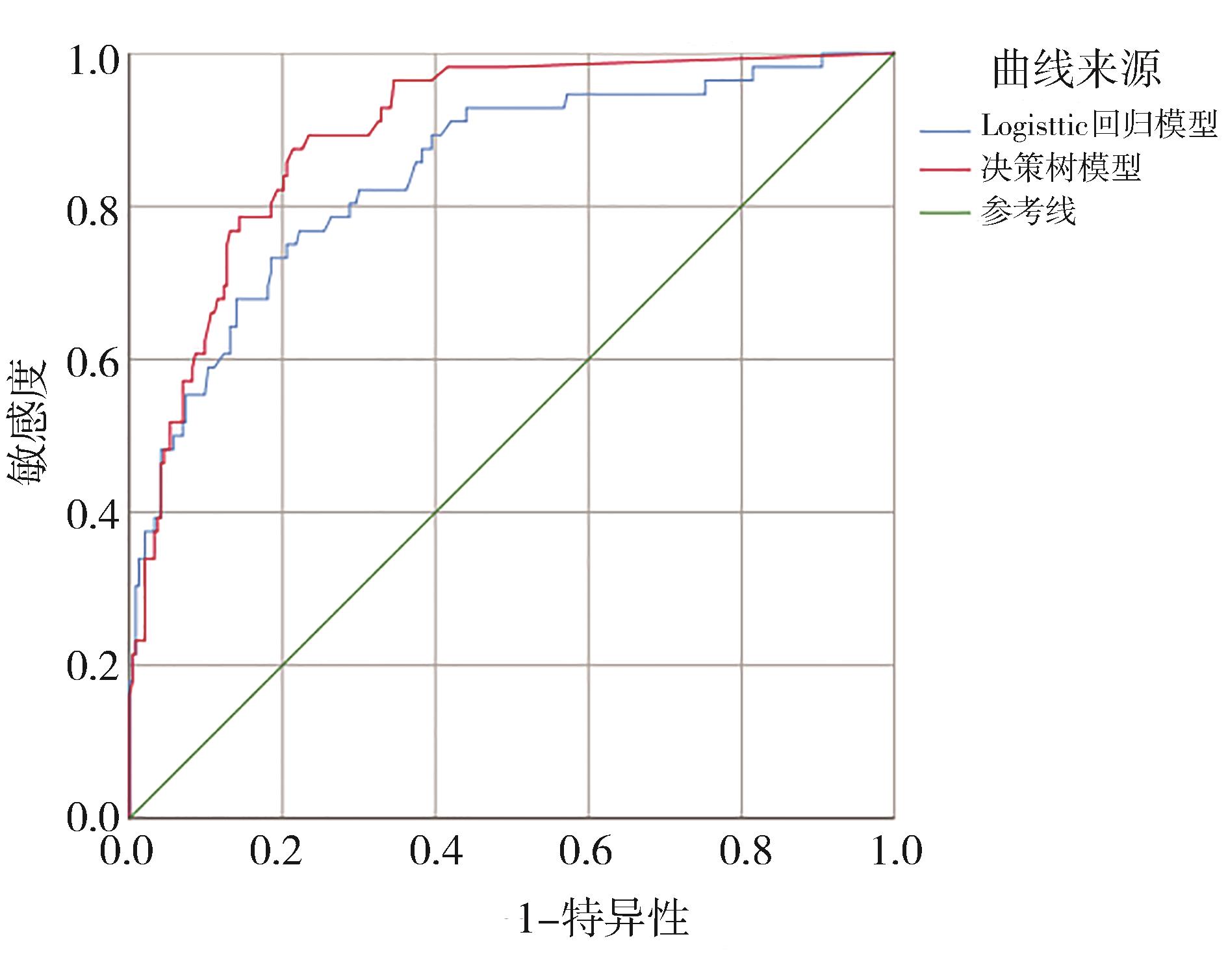
目的 探讨口腔癌游离皮瓣重建患者气管切开术后肺炎(POP)的危险因素,并基于Logistic回归模型和决策树模型构建口腔癌游离皮瓣重建患者POP的风险预测模型。 方法 回顾性收集2017年1月—2023年9月在中国西南地区3家医院行气管切开的299例口腔癌游离皮瓣重建患者的临床资料。采用多因素Logistic回归分析口腔癌游离皮瓣重建患者气管切开后POP的危险因素,运用SPSS Modeler18.0软件构建口腔癌游离皮瓣重建患者气管切开后POP的决策树模型,并评价2种模型的预测效能。 结果 共纳入299例患者,POP患者56例,POP发病率为18.73%。Logistic回归分析显示,气管套管留置时间[OR=1.097,95%CI(1.039,1.158)]、颌骨切除[OR=2.439,95%CI(1.084,5.484)]、吻合静脉数量[OR=3.345,95%CI(1.449,7.719)]和术后抗生素种类≥3[OR=14.732,95%CI(4.405,49.273)]是口腔癌游离皮瓣重建患者气管切开后发生POP的独立危险因素(P<0.05)。决策树模型显示,术后住院时间(>14 d)是口腔癌POP发生的主要危险因素,其次是吻合静脉数量、术后抗生素种类等。受试者工作特征曲线下面积显示,决策树模型的预测能力稍优于Logistic回归模型。 结论 口腔癌游离皮瓣患者POP的危险因素较多,决策树模型在本研究中对POP的预测效能稍好,临床可应用该模型了解口腔癌游离皮瓣重建患者气管切开后易发生POP的相关特征,并验证其预测效能。
中图分类号:
| [1] | Meier J, Wunschel M, Angermann A, et al. In-fluence of early elective tracheostomy on the incidence of postoperative complications in patients under-going head and neck surgery[J]. BMC Anesthesiol, 2019, 19(1): 43. |
| [2] | Goetz C, Burian NM, Weitz J, et al. Temporary tracheotomy in microvascular reconstruction in maxillofacial surgery: benefit or threat[J]. J Craniomaxillofac Surg, 2019, 47(4): 642-646. |
| [3] | 邢为刚. 气管切开术对口腔颌面部肿瘤皮瓣修复患者术后肺部感染的影响[D]. 济南: 山东大学, 2019. |
| Xing WG. The effect of tracheotomy on patients with postoperative pulmonary infection after oral and maxillofacial free flap reconstruction[D]. Jinan: Shandong University, 2019. | |
| [4] | 蔡天怡, 章文博, 于尧, 等. 头颈部游离组织瓣移植术后预防性气管切开的临床分析[J]. 北京大学学报(医学版), 2022, 54(2): 363-368. |
| Cai TY, Zhang WB, Yu Y, et al. Clinical analysis of selective tracheostomy necessary for patients undergoing head and neck surgery with free flap reconstruction[J]. J Peking Univ (Med Ed), 2022, 54(2): 363-368. | |
| [5] | 李春洁, 毕小琴, 朱桂全. 口腔颌面部肿瘤患者游离皮瓣修复术的并发症预防及处理[J]. 国际口腔医学杂志, 2023, 50(2): 127-137. |
| Li CJ, Bi XQ, Zhu GQ. Complications prevention and treatment after free flap reconstructive surgery for oral and maxillofacial tumor patients[J]. Int J Stomatol, 2023, 50(2): 127-137. | |
| [6] | Xu JY, Hu J, Yu P, et al. Perioperative risk factors for postoperative pneumonia after major oral cancer surgery: a retrospective analysis of 331 cases[J]. PLoS One, 2017, 12(11): e0188167. |
| [7] | Lai CJ, Shih PY, Cheng YJ, et al. Incidence and risk factors of postoperative pulmonary complications after oral cancer surgery with free flap reconstruction: a single center study[J]. J Formos Med Assoc, 2024, 123(3): 347-356. |
| [8] | Karthik K, Dhiwakar M. Predictors of surgical site infection and pneumonia following oral cavity tumor surgery[J]. Head Neck, 2021, 43(10): 3106-3115. |
| [9] | Reddy PD, Yan F, Nguyen SA, et al. Factors in-fluencing the development of pneumonia in patients with head and neck cancer: a meta-analysis[J]. Otolaryngol Head Neck Surg, 2021, 164(2): 234-243. |
| [10] | 刘迷迷, 刘永佳, 温丽, 等. C 5.0决策树对早期胃癌风险筛查研究[J]. 中华肿瘤防治杂志, 2018, 25(16): 1131-1135. |
| Liu MM, Liu YJ, Wen L, et al. Screening the risk of early gastric cancer based on C 5.0 decision tree[J]. Chin J Cancer Prev Treat, 2018, 25(16): 1131-1135. | |
| [11] | 苗若琪, 乔瑞萍, Effah CY, 等. 基于数据挖掘技术的社区获得性肺炎患病风险预测模型的构建[J]. 郑州大学学报(医学版), 2023, 58(3): 306-310. |
| Miao RQ, Qiao RP, Effah CY, et al. Application of data mining technology in prevalence risk model for community-acquired pneumonia[J]. J Zhengzhou Univ (Med Ed), 2023, 58(3): 306-310. | |
| [12] | 张燕, 彭伶丽, 张磊, 等. 基于logistic回归和决策树法预测颅脑肿瘤患者术后病情恶化风险[J]. 护理学杂志, 2022, 37(7): 15-19. |
| Zhang Y, Peng LL, Zhang L, et al. Risk prediction of postoperative deterioration for patients with craniocerebral tumors based on logistic regression and decision tree method[J]. J Nurs, 2022, 37(7): 15-19. | |
| [13] | 中华人民共和国卫生部. 医院感染诊断标准(试行)[J]. 中华医学杂志, 2001, 81(5): 314-320. |
| Ministry of Health of the People’s Republic of China. Diagnostic criteria for hospital infections (trial)[J]. Natl Med J China, 2001, 81(5): 314-320. | |
| [14] | Hey C, Goeze A, Sader R, et al. FraMaDySc: dysphagia screening for patients after surgery for head and neck cancer[J]. Eur Arch Otorhinolaryngol, 2023, 280(5): 2585-2592. |
| [15] | Skoretz SA, Anger N, Wellman L, et al. A systematic review of tracheostomy modifications and swallo-wing in adults[J]. Dysphagia, 2020, 35(6): 935-947. |
| [16] | Sood R, Paul J, Rajan S. Predictors of postoperative pneumonia in patients undergoing oral cancer resections and its management[J]. J Head Neck Phys Surg, 2018, 6(2): 69-72. |
| [17] | Matsumura Y, Sugiyama T, Kondo N, et al. Fluid restriction management in the treatment of COVID-19: a single-center observational study[J]. Sci Rep, 2022, 12(1): 17339. |
| [18] | Yeung JK, Harrop R, McCreary O, et al. Delayed mobilization after microsurgical reconstruction: an independent risk factor for pneumonia[J]. Laryngoscope, 2013, 123(12): 2996-3000. |
| [19] | Li L, Yuan WJ, Zhang SL, et al. Analysis of risk factors for pneumonia in 482 patients undergoing oral cancer surgery with tracheotomy[J]. J Oral Maxillofac Surg, 2016, 74(2): 415-419. |
| [20] | Pecorari G, Riva G, Albera A, et al. Post-operative infections in head and neck cancer surgery: risk factors for different infection sites[J]. J Clin Med, 2022, 11(17): 4969. |
| [21] | 杨迪. 口腔颌面部恶性肿瘤患者行预防性气管切开术后并发肺部感染的相关危险因素分析[D]. 大连: 大连医科大学, 2021. |
| Yang D. Analysis of relevant risk factors for pulmonary infection in patients with oral and maxillofacial malignancies after prophylactic tracheotomy[D]. Da-lian: Dalian Medical University, 2021. | |
| [22] | Riekert M, Rempel V, Keilwerth S, et al. Airway-associated complications with and without primary tracheotomy in oral squamous cell carcinoma surgery[J]. J Craniofac Surg, 2023, 34(1): 279-283. |
| [23] | Meier J, Wunschel M, Angermann A, et al. In-fluence of early elective tracheostomy on the incidence of postoperative complications in patients undergoing head and neck surgery[J]. BMC Anesthesiol, 2019, 19(1): 43. |
| [24] | 中华医学会呼吸病学分会感染学组. 中国成人医院获得性肺炎与呼吸机相关性肺炎诊断和治疗指南(2018年版)[J]. 中华结核和呼吸杂志, 2018, 41(4): 255-280. |
| The Infectious Diseases Group of the Respiratory Branch of the Chinese Medical Association. Diagnosis and treatment guidelines for chinese adult hospital acquired pneumonia and ventilator associated pneumonia (2018 Edition)[J]. Chin J Tuberc Respir Dis, 2018, 41(4): 255-280. | |
| [25] | 尹寿成, 徐中飞. 头颈部缺损修复重建中受区静脉的比较分析[J]. 口腔医学研究, 2020, 36(11): 1004-1006. |
| Yin SC, Xu ZF. Comparative analysis of recipient veins in reconstruction of head and neck defects[J]. J Oral Sci Res, 2020, 36(11): 1004-1006. | |
| [26] | Han ZX, Li JZ, Li H, et al. Single versus dual venous anastomoses of the free fibula osteocutaneous flap in mandibular reconstruction: a retrospective study[J]. Microsurgery, 2013, 33(8): 652-655. |
| [27] | Brady JS, Desai SV, Crippen MM, et al. Association of anesthesia duration with complications after microvascular reconstruction of the head and neck[J]. JAMA Facial Plast Surg, 2018, 20(3): 188-195. |
| [28] | 苏俊琪, 宋扬, 谢尚. 口腔鳞状细胞癌患者修复重建术后感染的病原学特征及感染风险预测模型的构建[J]. 北京大学学报(医学版), 2022, 54(1): 68-76. |
| Su JQ, Song Y, Xie S. Analysis of etiological characteristics and establishment of prediction model of postoperative infections in patients undergoing oral squamous cell carcinoma surgery with free flap reconstruction[J]. J Peking Univ (Med Ed), 2022, 54(1): 68-76. | |
| [29] | 顾徐嘉, 孟箭, 李志萍. 头颈部恶性肿瘤根治术预防性气管切开并发肺部感染危险因素及其预测模型构建[J]. 中华医院感染学杂志, 2024, 34(5): 727-732. |
| Gu XJ, Meng J, Li ZP. Risk factors for pulmonary infection in patients with head and neck malignant tumors undergoing radical surgery and preventive tracheotomy and establishment of prediction model[J]. Chin J Nosocomiol, 2024, 34(5): 727-732. |
| [1] | 曹梦颖,石蕊,于瀚雯,刘程程. 遥感成像技术在口腔疾病诊疗应用的研究进展[J]. 国际口腔医学杂志, 2025, 52(1): 107-116. |
| [2] | 符天宇,张雪,王思琪,郭程祎,董晓宇,程亚鹏,李锐. 碳点在口腔颌面部恶性肿瘤的诊断及治疗中的应用[J]. 国际口腔医学杂志, 2025, 52(1): 25-33. |
| [3] | 吴媚, 梁妍景, 彭雪沛, 陈卫宏, 郭星铜, 侯黎莉. 口腔癌术后言语功能影响因素分析[J]. 国际口腔医学杂志, 2025, 52(1): 42-49. |
| [4] | 廖永珍, 王晓辉, 邱洁, 周加靓, 丛丽. 2003—2023年口腔癌智慧医疗文献循证可视化及对比分析[J]. 国际口腔医学杂志, 2025, 52(1): 50-60. |
| [5] | 傅豫, 何薇, 黄兰. 铁死亡在口腔疾病中的研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 36-44. |
| [6] | 姜玥莹,何宇添,李婷,周蓉卉. 近红外荧光探针在口腔癌诊断中应用的研究进展[J]. 国际口腔医学杂志, 2023, 50(4): 407-413. |
| [7] | 范琳,孙江. 微针在口腔医学中的应用[J]. 国际口腔医学杂志, 2023, 50(4): 472-478. |
| [8] | 林慧平,徐婷,林军. 人工智能在口腔癌和口腔潜在恶性疾病诊断中的研究进展[J]. 国际口腔医学杂志, 2023, 50(2): 138-145. |
| [9] | 王太萍,石兴莲,李喆臻,刘梅,姜健红. 口腔癌患者心理因素及干预现状分析[J]. 国际口腔医学杂志, 2023, 50(2): 203-209. |
| [10] | 陈荟宇,白明茹,叶玲. 信号素3A与口腔常见病关系的研究进展[J]. 国际口腔医学杂志, 2022, 49(5): 593-599. |
| [11] | 黄璐,戴杰,吴燕岷. 唾液生物标志物在口腔癌筛查中的应用[J]. 国际口腔医学杂志, 2020, 47(1): 68-75. |
| [12] | 原振英,管翠强,南欣荣. DNA甲基化与口腔疾病的研究进展[J]. 国际口腔医学杂志, 2019, 46(4): 437-441. |
| [13] | 李倩,张平,陈娇,曾昕,冯云. 唾液组学在口腔癌诊断中的应用[J]. 国际口腔医学杂志, 2018, 45(6): 710-715. |
| [14] | 韩曈曈,陈乔尔,朱友明. p53相关长链非编码RNA及其与口腔癌的关系[J]. 国际口腔医学杂志, 2018, 45(5): 597-602. |
| [15] | 屈茜1 房付春1 吴补领1,2. 长链非编码RNA在牙周炎和口腔肿瘤疾病中的作用[J]. 国际口腔医学杂志, 2016, 43(1): 62-. |
|
||