国际口腔医学杂志 ›› 2023, Vol. 50 ›› Issue (3): 272-278.doi: 10.7518/gjkq.2023054
万雪丽1( ),石永乐2,张秀芬1,王欢1,田莉1()
),石永乐2,张秀芬1,王欢1,田莉1()
Wan Xueli1(),Shi Yongle2,Zhang Xiufen1,Wang Huan1,Tian Li1()
摘要:
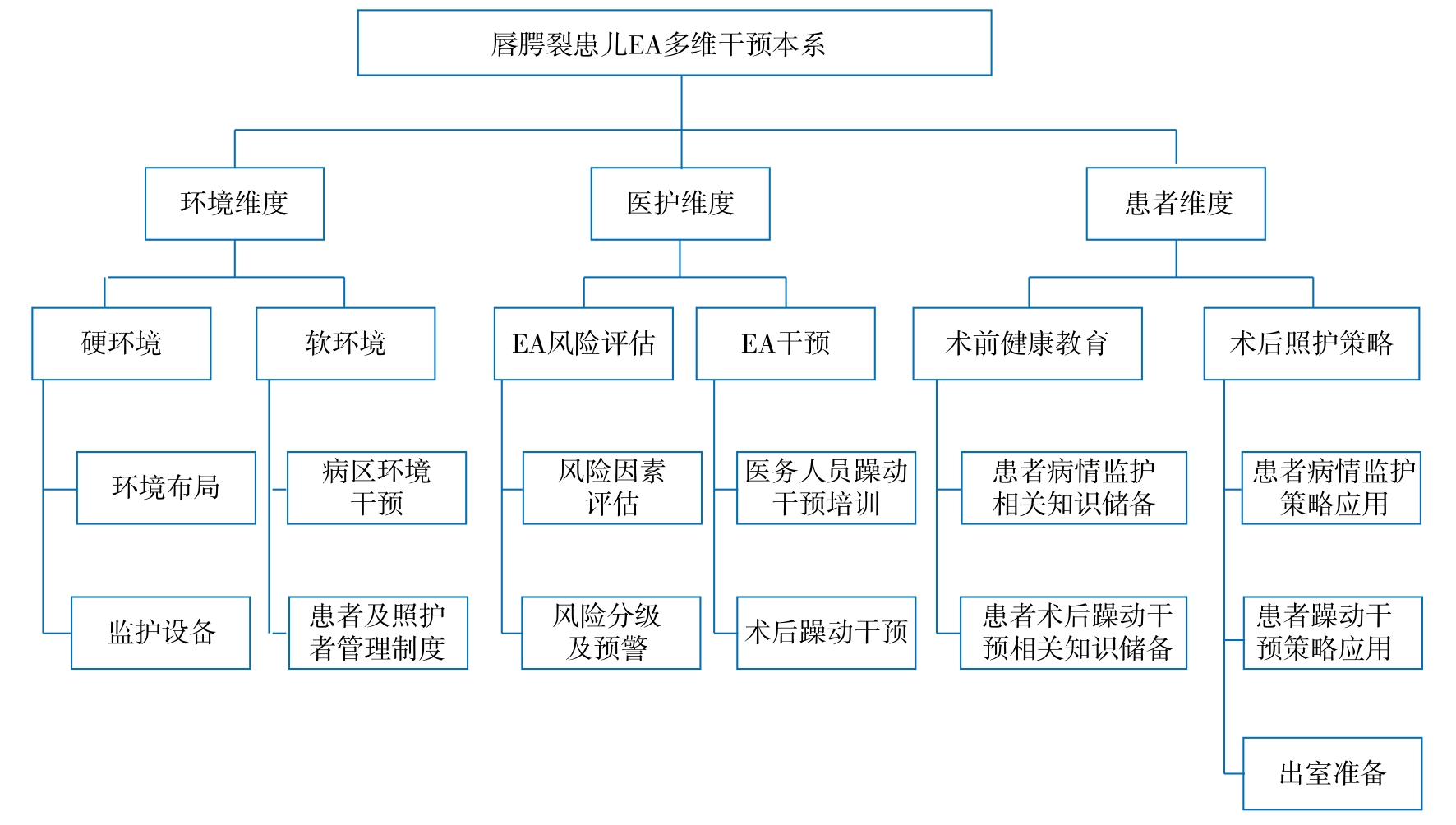
目的 构建并应用唇腭裂患儿全身麻醉苏醒期躁动(EA)多维干预体系,以降低唇腭裂患儿EA发生率。 方法 专家函询法构建唇腭裂患儿EA多维干预体系。便利选取2021年11月—2022年6月入住四川大学华西口腔医院麻醉复苏室(PACU)的唇腭裂患儿119例,分试验组59例和对照组60例,试验组应用唇腭裂患儿EA多维干预体系干预,对照组常规干预,采用儿童麻醉苏醒期谵妄量表(PAED)及疼痛评估量表(FLACC)评估干预效果。 结果 唇腭裂患儿EA多维干预体系包括3项一级指标、6项二级指标、14项三级指标。试验组在PACU内、转出PACU的躁动发生率低于对照组(P<0.05),两组术后生命体征、FLACC疼痛评分及并发症的发生率差异无统计学意义(P>0.05)。 结论 唇腭裂患儿EA多维干预体系具有科学性,可降低唇腭裂患儿EA的发生率,但对疼痛及术后并发症的发生尚无确定改善效果。
中图分类号:
| 1 | Denning S, Ng E, Wong Riff KWY. Anaesthesia for cleft lip and palate surgery[J]. BJA Educ, 2021, 21(10): 384-389. |
| 2 | Wang MY, Meng RG, Wang ZQ, et al. Prevalence of oral clefts among live births in Gansu province, China[J]. Int J Environ Res Public Health, 2018, 15(2): 380. |
| 3 | Salari N, Darvishi N, Heydari M, et al. Global pre-valence of cleft palate, cleft lip and cleft palate and lip: a comprehensive systematic review and meta-analysis[J]. J Stomatol Oral Maxillofac Surg, 2022, 123(2): 110-120. |
| 4 | Fan DZ, Wu SZ, Liu L, et al. Prevalence of non-syndromic orofacial clefts: based on 15 094 978 Chinese perinatal infants[J]. Oncotarget, 2018, 9(17): 13981-13990. |
| 5 | Yang XL, Hu ZY, Peng F, et al. Effects of dexmedetomidine on emergence agitation and recovery quality among children undergoing surgery under general anesthesia: a meta-analysis of randomized controlled trials[J]. Front Pediatr, 2020, 8: 580226. |
| 6 | Moore AD, Anghelescu DL. Emergence delirium in pediatric anesthesia[J]. Paediatr Drugs, 2017, 19(1): 11-20. |
| 7 | Shi YL, Zhang XF, Sun Y, et al. Emergence agitation after the cleft lip or palate surgery in pediatric patients: a prospective study[J]. J Stomatol Oral Maxillofac Surg, 2021, 122(6): 539-543. |
| 8 | Eshetie D, Getinet H, Abdissa Z, et al. Incidence and associated factors of emergence agitation after general anesthesia and surgery among pediatric patients: a prospective follow-up study[J]. Int J Surg Open, 2020, 27: 25-31. |
| 9 | Xu H, Mei XP, Xu LX. Cause analysis, prevention, and treatment of postoperative restlessness after ge-neral anesthesia in children with cleft palate[J]. J Dent Anesth Pain Med, 2017, 17(1): 13-20. |
| 10 | 唇腭裂多学科协作诊疗专家组, 贾仲林, 石冰, 等. 唇腭裂孕前-产前-产后多学科协作诊疗流程专家共识[J]. 中华口腔医学杂志, 2021(11): 1059-1065. |
| Expert Group of Multidisciplinary Treatment Process of Cleft Lip and Palate, Jia ZL, Shi B, et al. Specification of the multidisciplinary treatment process of cleft lip and palate during pregnancy, prenatal and postnatal stages[J]. Chin J Stomatol, 2021(11): 1059-1065. | |
| 11 | Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale[J]. Anesthesiology, 2004, 100(5): 1138-1145. |
| 12 | Ringblom J, Wåhlin I, Proczkowska M. A psychometric evaluation of the pediatric anesthesia emergence delirium scale[J]. PaediatrAnaesth, 2018, 28(4): 332-337. |
| 13 | Merkel SI, Voepel-Lewis T, Shayevitz JR, et al. The FLACC: a behavioral scale for scoring postoperative pain in young children[J]. Pediatr Nurs, 1997, 23(3): 293-297. |
| 14 | 刘明, 陈利琴, 郑佳丽. 儿童疼痛行为量表在唇腭裂患儿术后疼痛评估中的应用及其信效度[J]. 解放军护理杂志, 2012, 29(13): 20-22, 26. |
| Liu M, Chen LQ, Zheng JL. The appraisal of re-liability and validity of the FLACC observation tool for scoring painfulness of children with cleft lip and palate[J]. Nurs J Chin People’s Liberation Army, 2012, 29(13): 20-22, 26. | |
| 15 | Lee SJ, Sung TY. Emergence agitation: current knowledge and unresolved questions[J]. Korean J Anesthesiol, 2020, 73(6): 471-485. |
| 16 | 卢露, 卢芳燕, 张婉莹, 等. 童趣化护理在危重住院患儿护理中的应用进展[J]. 中华急危重症护理杂志, 2022, 3(5): 477-480. |
| Lu L, Lu FY, Zhang WY, et al. Research progress on the application of childlike nursing in the nursing of critically ill hospitalized children[J]. Chin J Emerg Crit Care Nurs, 2022, 3(5): 477-480. | |
| 17 | 张文光, 武婵媛, 陆欣, 等. 住院患者护理风险评估与管理的研究进展[J]. 当代医学, 2016, 22(25): 11-13. |
| Zhang WG, Wu CY, Lu X, et al. Research progress on nursing risk assessment and management of inpatients[J]. Contemp Med, 2016, 22(25): 11-13. | |
| 18 | 贾会英, 梁靖, 周梦, 等. 患儿全身麻醉苏醒期躁动及父母陪伴对其影响的研究进展[J]. 中华护理杂志, 2016, 51(10): 1230-1233. |
| Jia HY, Liang J, Zhou M, et al. Research progress on the influence of restlessness and parental companionship on children during recovery from gene-ral anesthesia[J]. Chin J Nurs, 2016, 51(10): 1230-1233. |
| [1] | 夏溦瑶,贾仲林. 维生素与唇腭裂发生相关性的研究进展[J]. 国际口腔医学杂志, 2023, 50(6): 632-638. |
| [2] | 陈卓,石冰,李精韬. 唇腭裂患者外鼻生长特征的研究进展[J]. 国际口腔医学杂志, 2023, 50(3): 279-286. |
| [3] | 裴玲,曾妮,杨超,何苗,罗强,石冰,郑谦. 辅助局部麻醉对唇腭裂整复术后镇痛效果的研究[J]. 国际口腔医学杂志, 2022, 49(6): 657-662. |
| [4] | 黄艺璇,石冰,李精韬. 唇腭裂患者鼻通气功能的研究进展[J]. 国际口腔医学杂志, 2022, 49(4): 453-461. |
| [5] | 张琦,范存晖,杨茜,李然,徐晓琳,丁玮,王文惠,杨彩秀. 替牙期骨性Ⅲ类单侧完全性唇腭裂与非唇腭裂患者牙弓形态的对比研究[J]. 国际口腔医学杂志, 2022, 49(2): 144-152. |
| [6] | 孙嘉琳,林岩松,石冰,贾仲林. 5种常见综合征型唇腭裂遗传学研究进展[J]. 国际口腔医学杂志, 2021, 48(6): 718-724. |
| [7] | 马晓芳,黄永清,石冰,马坚. 双生子模型在唇腭裂病因学研究中的应用[J]. 国际口腔医学杂志, 2021, 48(5): 512-519. |
| [8] | 吴敏,石冰. 唇腭裂婴儿母乳喂养的研究进展[J]. 国际口腔医学杂志, 2021, 48(3): 269-273. |
| [9] | 侯亚丽,马利. 亚洲人群干扰素调节因子6基因多态性与非综合征型唇腭裂相关性研究的Meta分析[J]. 国际口腔医学杂志, 2020, 47(4): 397-405. |
| [10] | 宋少华,莫水学. 唇腭裂患者序列治疗中的正畸治疗[J]. 国际口腔医学杂志, 2019, 46(6): 740-744. |
| [11] | 邓程丹,石冰,李杨. 唇腭裂患者的脑部结构与功能研究进展[J]. 国际口腔医学杂志, 2019, 46(5): 617-620. |
| [12] | 刘丹,毛渤淳,雒如燕,崔珂,石冰,龚彩霞. 唇腭裂患者家庭抗逆力及其影响因素[J]. 国际口腔医学杂志, 2019, 46(3): 297-301. |
| [13] | 刘育豪,白娜,程梦龙,石冰,李芷慧,龚彩霞. 视频示范法对围手术期唇腭裂患儿父母的心理干预效果分析[J]. 国际口腔医学杂志, 2019, 46(1): 26-29. |
| [14] | 蒲泓伶, 陈丽先, 龚彩霞, 吴敏, 石冰. 0~6岁唇腭裂患儿血液生化指标的变化规律[J]. 国际口腔医学杂志, 2017, 44(4): 385-389. |
| [15] | 宋蕾, 姜舒原, 贾仲林, 石冰, 龚彩霞, 李杨. 唇腭裂患儿术前上呼吸道感染相关症状对术后生命体征影响的初步分析[J]. 国际口腔医学杂志, 2017, 44(4): 398-404. |
|