国际口腔医学杂志 ›› 2024, Vol. 51 ›› Issue (6): 722-727.doi: 10.7518/gjkq.2024068
• 论著 • 上一篇
毛奇蓉( ),尹恒,吴敏,石冰,郑谦,李精韬()
),尹恒,吴敏,石冰,郑谦,李精韬()
Qirong Mao(),Heng Yin,Min Wu,Bing Shi,Qian Zheng,Jingtao Li()
摘要:
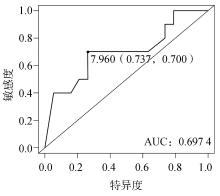
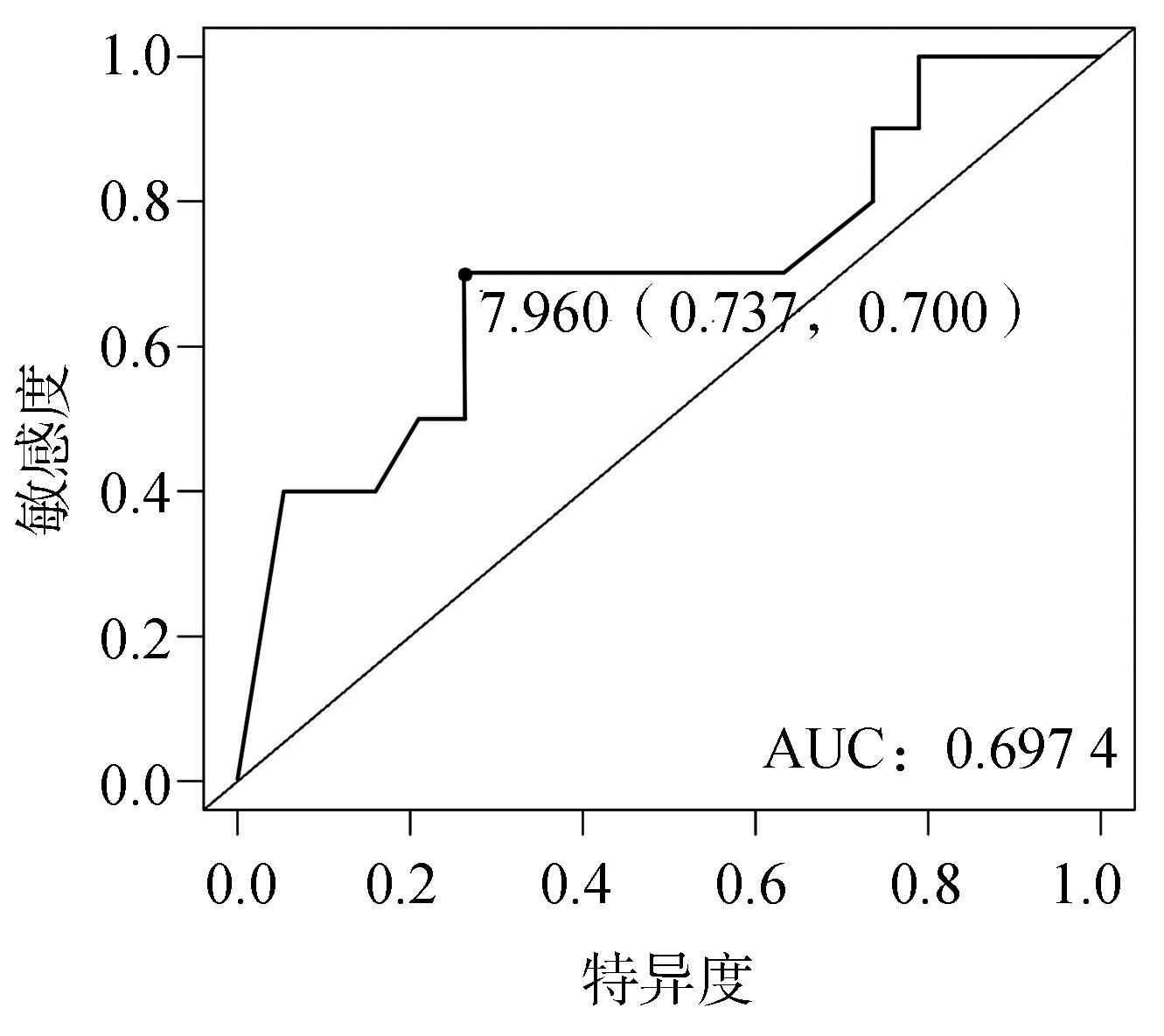
目的 探讨对腭裂术后边缘性腭咽闭合不全(MVPI)患者进行语音训练的可行性及预后因素分析。 方法 对腭裂术后确诊为MVPI并接受语音训练的患者进行了回访。对比治疗前后患者的语音情况评估语音训练的效果。分别进行单因素和多因素逻辑回归检验,分析语音训练后MVPI治疗效果的影响因素。 结果 语音训练能明显改善患者的高鼻音、构音和语音清晰度,但未能明显改善患者的鼻漏气。逻辑回归分析表明,治疗时的年龄是影响预后的重要因素。8岁以上患者的语音训练有效率(17.6%)明显低于8岁以下患者(58.3%)。 结论 语音训练是改善MVPI患者语音清晰度的有效治疗方法,年龄和是否存在鼻漏气可能是影响MVPI语音训练效果的关键因素。
中图分类号:
| 1 | Ruda JM, Krakovitz P, Rose AS. A review of the evaluation and management of velopharyngeal insufficiency in children[J]. Otolaryngol Clin North Am, 2012, 45(3): 653-669. |
| 2 | Johns DF, Rohrich RJ, Awada M. Velopharyngeal incompetence: a guide for clinical evaluation[J]. Plast Reconstr Surg, 2003, 112(7): 1890-1898, 1982. |
| 3 | Lindeborg MM, Shakya P, Rai SM, et al. Optimi-zing speech outcomes for cleft palate[J]. Curr Opin Otolaryngol Head Neck Surg, 2020, 28(4): 206-211. |
| 4 | Harding A, Grunwell P. Active versus passive cleft-type speech characteristics[J]. Int J Lang Commun Disord, 1998, 33(3): 329-352. |
| 5 | Smith B, Guyette TW. Evaluation of cleft palate speech[J]. Clin Plast Surg, 2004, 31(2): 251-260. |
| 6 | Henningsson G, Kuehn DP, Sell D, et al. Universal parameters for reporting speech outcomes in indivi-duals with cleft palate[J]. Cleft Palate Craniofac J, 2008, 45(1): 1-17. |
| 7 | Hu HM, Xi X, Wong LLN, et al. Construction and evaluation of the Mandarin Chinese matrix (CMNmatrix) sentence test for the assessment of speech recognition in noise[J]. Int J Audiol, 2018, 57(11): 838-850. |
| 8 | 马平川, 毛渤淳, 郭春丽, 等. 汉语普通话腭裂语音数据库的搭建与应用[J]. 华西口腔医学杂志, 2020, 38(2): 149-154. |
| Ma PC, Mao BC, Guo CL, et al. Establishment and application of mandarin cleft palate speech database[J]. West China J Stomatol, 2020, 38(2): 149-154. | |
| 9 | Zhang B, Guo CL, Yin H, et al. The correlation between consonant articulation and velopharyngeal function in patients with unoperated submucous cleft palate[J]. J Craniofac Surg, 2020, 31(4): 1070-1073. |
| 10 | Zhang B, Yang C, Yin H, et al. Preoperative velopharyngeal closure ratio correlates with Furlow palatoplasty outcome among patients with nonsyndro-mic submucous cleft palate[J]. J Craniomaxillofac Surg, 2020, 48(10): 962-968. |
| 11 | Cheng X, Bo ZY, Yin H, et al. Age and preoperative velar closure ratio are significantly associated with surgical outcome of furlow double-opposing Z-plasty in palatal re-repair[J]. J Oral Maxillofac Surg, 2020, 78(3): 431-439. |
| 12 | 尹恒, 郭春丽, 石冰, 等. 黏膜下腭裂的形态分类与腭咽功能分析[J]. 华西口腔医学杂志, 2016, 34(5): 488-492. |
| Yin H, Guo CL, Shi B, et al. Morphological classification and velopharyngeal function analysis of submucous cleft palate patients[J]. West China J Stomatol, 2016, 34(5): 488-492. | |
| 13 | 马思维, 任战平, 文抑西, 等. 65例腭裂术后MVPI患者构音特点及治疗策略探讨[J]. 实用口腔医学杂志, 2013, 29(6): 844-847. |
| Ma SW, Ren ZP, Wen YX, et al. Articulation of 65 patients with MVPI and the speech therapy approach after repair of cleft palate[J]. J Pract Stomatol, 2013, 29(6): 844-847. | |
| 14 | 毛奇蓉, 尹恒, 李精韬. 边缘性腭咽闭合不全临床诊疗研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 116-123. |
| Mao QR, Yin H, Li JT. Progress in the management of marginal velopharyngeal incompetence[J]. Int J Stomatol, 2024, 51(1): 116-123. | |
| 15 | Krause CJ, Tharp RF, Morris HL. A comparative study of results of the von Langenbeck and the V-Y pushback palatoplasties[J]. Cleft Palate J, 1976, 13: 11-19. |
| 16 | Neely BJ, Bradley DP. A rating scale for evaluation of video tape recorded X-ray studies[J]. Cleft Palate J, 1964, 16: 88-94. |
| 17 | Laine T, Warren DW, Dalston RM, et al. Screening of velopharyngeal closure based on nasal airflow rate measurements[J]. Cleft Palate J, 1988, 25(3): 220-225. |
| 18 | Warren DW, Dalston RM, Mayo R. Hypernasality and velopharyngeal impairment[J]. Cleft Palate Craniofac J, 1994, 31(4): 257-262. |
| 19 | Morris HL, Smith JK. A multiple approach for eva-luating velopharyngeal competency[J]. J Speech Hear Disord, 1962, 27: 218-226. |
| 20 | Smith BE, Guyette TW. Pressure-flow differences in performance during production of the CV syllables /pi/ and /pa/[J]. Cleft Palate Craniofac J, 1996, 33(1): 74-76. |
| 21 | Warren DW, Dalston RM, Mayo R. Hypernasality in the presence of “adequate” velopharyngeal closure[J]. Cleft Palate Craniofac J, 1993, 30(2): 150-154. |
| 22 | Jones DL, Morris HL, Van Demark DR. A comparison of oral-nasal balance patterns in speakers who are categorized as “almost but not quite” and “sometimes but not always”[J]. Cleft Palate Craniofac J, 2004, 41(5): 526-534. |
| 23 | Murthy J, Sendhilnathan S, Hussain SA. Speech outcome following late primary palate repair[J]. Cleft Palate Craniofac J, 2010, 47(2): 156-161. |
| 24 | Pamplona C, Ysunza A, Patiño C, et al. Speech summer camp for treating articulation disorders in cleft palate patients[J]. Int J Pediatr Otorhinolaryngol, 2005, 69(3): 351-359. |
| 25 | Derakhshandeh F, Nikmaram M, Hosseinabad HH, et al. Speech characteristics after articulation therapy in children with cleft palate and velopharyngeal dysfunction-a single case experimental design[J]. Int J Pediatr Otorhinolaryngol, 2016, 86: 104-113. |
| [1] | 徐一尘,鲁勇. 腭裂术后瘘修复的研究进展[J]. 国际口腔医学杂志, 2024, 51(5): 624-629. |
| [2] | 李亚楠,石冰,李精韬. 咽后壁瓣咽成形术相关通气功能障碍及应对[J]. 国际口腔医学杂志, 2024, 51(2): 233-240. |
| [3] | 毛奇蓉,尹恒,李精韬. 边缘性腭咽闭合不全临床诊疗研究进展[J]. 国际口腔医学杂志, 2024, 51(1): 116-124. |
| [4] | 夏溦瑶,贾仲林. 维生素与唇腭裂发生相关性的研究进展[J]. 国际口腔医学杂志, 2023, 50(6): 632-638. |
| [5] | 万雪丽,石永乐,张秀芬,王欢,田莉. 唇腭裂患儿全身麻醉苏醒期躁动多维干预体系的构建研究[J]. 国际口腔医学杂志, 2023, 50(3): 272-278. |
| [6] | 陈卓,石冰,李精韬. 唇腭裂患者外鼻生长特征的研究进展[J]. 国际口腔医学杂志, 2023, 50(3): 279-286. |
| [7] | 石佳鑫,王淳艺,李精韬. Pierre Robin序列征患者腭裂临床治疗的研究进展[J]. 国际口腔医学杂志, 2023, 50(2): 237-242. |
| [8] | 张宇宁,曾妮,张焙,石冰,郑谦. 咽后壁瓣咽成形术对腭裂术后患者颌面部生长影响的初步研究[J]. 国际口腔医学杂志, 2023, 50(1): 66-71. |
| [9] | 裴玲,曾妮,杨超,何苗,罗强,石冰,郑谦. 辅助局部麻醉对唇腭裂整复术后镇痛效果的研究[J]. 国际口腔医学杂志, 2022, 49(6): 657-662. |
| [10] | 黄艺璇,石冰,李精韬. 唇腭裂患者鼻通气功能的研究进展[J]. 国际口腔医学杂志, 2022, 49(4): 453-461. |
| [11] | 罗枭,蔡生青,石冰,李承浩. 2,3,7,8-四氯二苯二噁英诱导C57BL小鼠腭裂发病机制的研究[J]. 国际口腔医学杂志, 2022, 49(3): 317-323. |
| [12] | 张琦,范存晖,杨茜,李然,徐晓琳,丁玮,王文惠,杨彩秀. 替牙期骨性Ⅲ类单侧完全性唇腭裂与非唇腭裂患者牙弓形态的对比研究[J]. 国际口腔医学杂志, 2022, 49(2): 144-152. |
| [13] | 吴敏,李承浩,李扬,龚彩霞,石冰. 腭裂裂隙宽度与Sommerlad-Furlow法修复腭裂术后腭瘘发生率的关联研究[J]. 国际口腔医学杂志, 2021, 48(6): 640-643. |
| [14] | 孙嘉琳,林岩松,石冰,贾仲林. 5种常见综合征型唇腭裂遗传学研究进展[J]. 国际口腔医学杂志, 2021, 48(6): 718-724. |
| [15] | 马晓芳,黄永清,石冰,马坚. 双生子模型在唇腭裂病因学研究中的应用[J]. 国际口腔医学杂志, 2021, 48(5): 512-519. |
|
||