国际口腔医学杂志 ›› 2026, Vol. 53 ›› Issue (2): 145-154.doi: 10.7518/gjkq.2026120
• 专家笔谈 •
王美青( )
)
Meiqing Wang()
摘要:
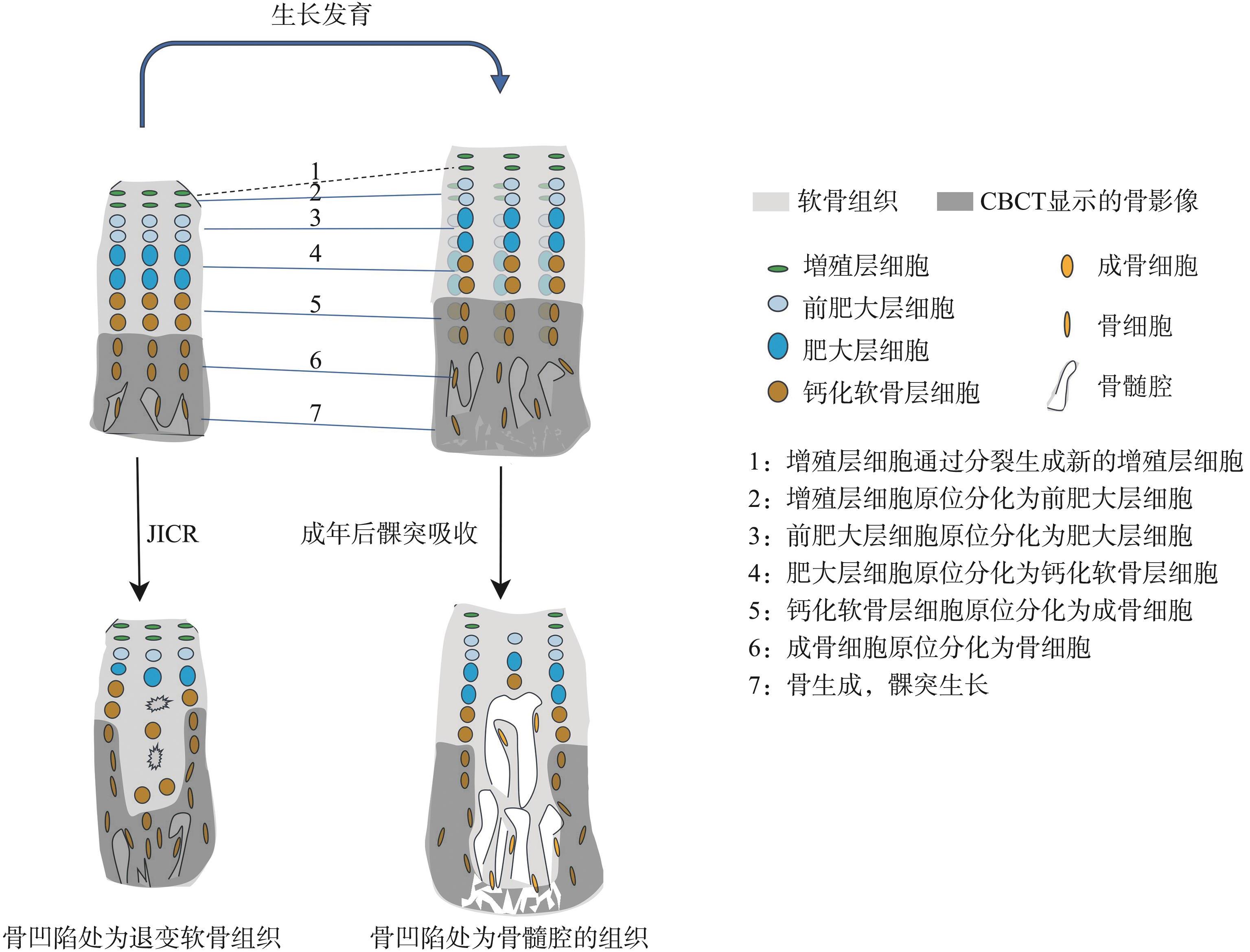
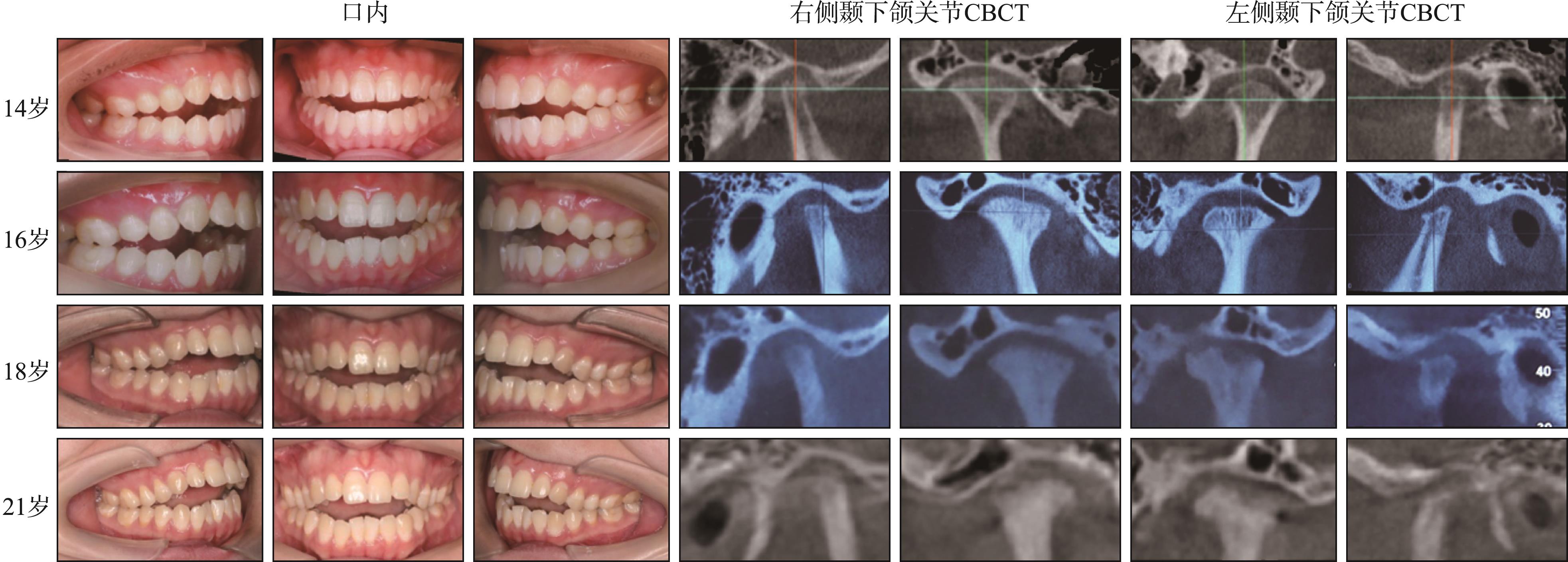
青少年特发性髁突吸收(JICR)是一种发病率较低的颞下颌关节疾病,以髁突组织进行性“吸收”为主要特征,造成患者下颌升支的高度降低、下颌后缩、前牙开𬌗等口颌面畸形。根据笔者研究团队的最新动物实验研究结果,与生长发育完成后出现的髁突吸收不同,JICR可能是发育期异常咬合所致关节软骨退变相关的髁突病理性改建。本文从文献所报道的病因、病理机理、诊断、鉴别诊断和治疗等方面,论证了这一观点:JICR的病因、病理机理尚未明确,损伤性负荷(包括异常咬合)具有一定的致病意义;目前JICR的诊断和治疗均存在很大的挑战性,确诊JICR主要依靠影像特征,但在早期影像特征尚不明显时,确诊该症比较困难,下颌后缩等Ⅱ类错𬌗畸形相关的颌面部畸形常被作为该症的早期表现之一;一些学者反对在JICR病变活跃期进行积极的治疗,认为此时的治疗有导致疾病加重的风险,但如果考虑到创伤性咬合的病因意义,推迟治疗可能导致错失最佳保守治疗时机、加剧髁突病变和口颌面畸形等问题。笔者认为,应尽快诊断和矫正造成该症的异常咬合,防止口颌面畸形的出现或加重。有效诊断和治疗咬合问题,成为解决JICR这一疑难疾病的关键。
中图分类号:
| [1] | Wolford LM, Cardenas L. Idiopathic condylar resorption: diagnosis, treatment protocol, and outco-mes[J]. Am J Orthod Dentofacial Orthop, 1999, 116(6): 667-677. |
| [2] | Young A. Idiopathic condylar resorption: the current understanding in diagnosis and treatment[J]. J In- dian Prosthodont Soc, 2017, 17(2): 128-135. |
| [3] | Nobrega MTC, Almeida FT, Friesen R, et al. Idiopathic condylar resorption in adolescents: a scoping review[J]. J Oral Rehabil, 2024, 51(8): 1610-1620. |
| [4] | Mercuri LG. Osteoarthritis, osteoarthrosis, and idiopathic condylar resorption[J]. Oral Maxillofac Surg Clin North Am, 2008, 20(2): 169-183. |
| [5] | Chamberland S. Progressive idiopathic condylar resorption: three case reports[J]. Am J Orthod Dentofacial Orthop, 2019, 156(4): 531-544. |
| [6] | Noh HK, Park HS. Considerations for vertical control with microimplants in a idiopathic condylar resorption patient: a case report[J]. J Orthod, 2021, 48(2): 172-182. |
| [7] | Kristensen KD, Schmidt B, Stoustrup P, et al. Idiopathic condylar resorptions: 3-dimensional condylar bony deformation, signs and symptoms[J]. Am J Orthod Dentofacial Orthop, 2017, 152(2): 214-223. |
| [8] | Lee GH, Park JH, Lee SM, et al. Orthodontic treatment protocols for patients with idiopathic condylar resorption[J]. J Clin Pediatr Dent, 2019, 43(4): 292-303. |
| [9] | Mitsimponas K, Mehmet S, Kennedy R, et al. Idiopathic condylar resorption[J]. Br J Oral Maxillofac Surg, 2018, 56(4): 249-255. |
| [10] | Mercuri LG, Handelman CS. Idiopathic condylar resorption: what should we do[J]. Oral Maxillofac Surg Clin North Am, 2020, 32(1): 105-116. |
| [11] | Tanaka E. Etiology and diagnosis for idiopathic condylar resorption in growing adolescents[J]. J Clin Med, 2023, 12(20): 6607. |
| [12] | Alsabban L, Amarista FJ, Mercuri LG, et al. Idiopathic condylar resorption: a survey and review of the literature[J]. J Oral Maxillofac Surg, 2018, 76(11): 2316.e1-2316.e13. |
| [13] | Sansare K, Raghav M, Mallya SM, et al. Management-related outcomes and radiographic findings of idiopathic condylar resorption: a systematic review[J]. Int J Oral Maxillofac Surg, 2015, 44(2): 209-216. |
| [14] | Roth S, Müller K, Fischer DC, et al. Specific properties of the extracellular chondroitin sulphate proteoglycans in the mandibular condylar growth centre in pigs[J]. Arch Oral Biol, 1997, 42(1): 63-76. |
| [15] | Tominaga K, Hirashima S, Fukuda J. An experimental model of osteoarthrosis of the temporomandibular joint in monkeys[J]. Br J Oral Maxillofac Surg, 2002, 40(3): 232-237. |
| [16] | Lovell NC. Skeletal and dental pathology of free-ranging mountain gorillas[J]. Am J Phys Anthropol, 1990, 81(3): 399-412. |
| [17] | Chen CP, Zhang JH, Zhang B, et al. Unilateral loss of maxillary molars in young mice leads to bilateral condylar adaptation and degenerative disease[J]. JB-MR Plus, 2022, 6(7): e10638. |
| [18] | Nogami S, Kataoka Y, Yamauchi K, et al. Condylar resorption following compressive mechanical stress in rabbit model‒association of matrix metalloproteinases[J]. In Vivo, 2022, 36(5): 2126-2133. |
| [19] | Nogami S, Yamauchi K, Odashima K, et al. Influen-ce of oestrogen deficiency and excessive mechanical stress on condylar head of mandible[J]. Oral Dis, 2020, 26(8): 1718-1726. |
| [20] | Yang HJ, Hwang SJ. Effects of 17β-estradiol deficiency and mechanical overload on osseous changes in the rat temporomandibular joint[J]. J Oral Maxillofac Surg, 2020, 78(2): 214.e1-214.e14. |
| [21] | Iwasaki T, Takahara N, Duc VV, et al. Effect of anterior disc displacement and estrogen deficiency on rabbit mandibular condyle[J]. J Oral Biosci, 2025, 67(1): 100599. |
| [22] | Jiao K, Dai J, Wang MQ, et al. Age- and sex-related changes of mandibular condylar cartilage and subchondral bone: a histomorphometric and micro-CT study in rats[J]. Arch Oral Biol, 2010, 55(2): 155-163. |
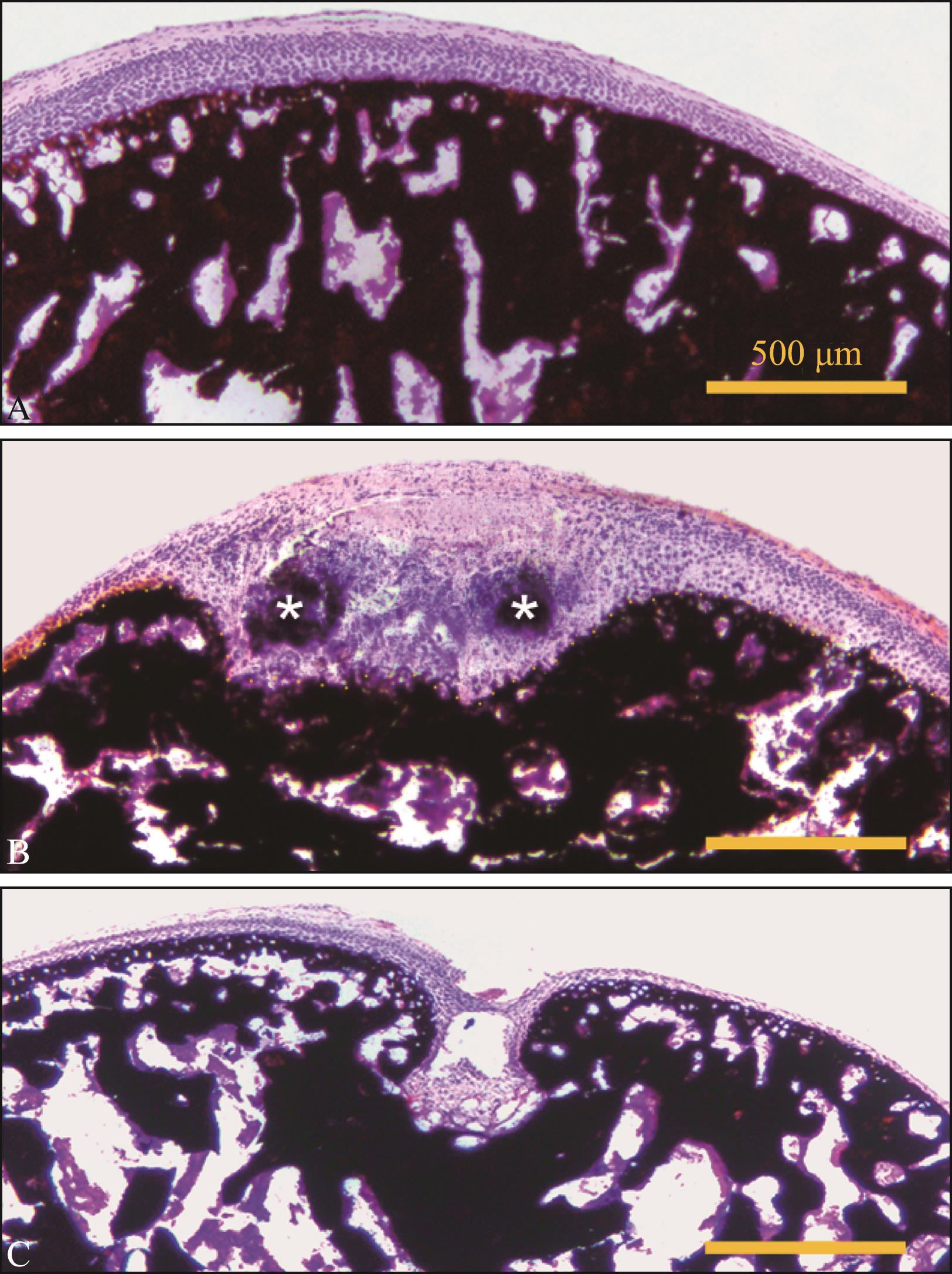
| [23] | Zhang YJ, Zhang J, Xu LF, et al. Unbalanced cartilage calcification during development contributes to the formation of irregular articular surfaces as revealed by micro-CT images[J]. Australas Orthod J, 2023, 39(2): 40-48. |
| [24] | 张月姣, 徐小杰, 刘倩, 等. 偏颌大鼠模型的构建及其髁突CT影像和组织学评价[J]. 口腔颌面外科杂志, 2021, 31(5): 278-284. |
| Zhang YJ, Xu XJ, Liu Q, et al. Construction of the mandible deviation occlusion rat model and micro-CT radiography and histology evaluation of the mandibular condyles[J]. J Oral Maxillofac Surg, 2021, 31(5): 278-284. | |
| [25] | Alali YS, Al Habeeb KM, Al Malhook KA, et al. Diagnosis and management of idiopathic condylar resorption: a review of literature[J]. Saudi Dent J, 2024, 36(11): 1397-1405. |
| [26] | Valladares-Neto J, Acioli GR, Teodoro AB, et al. Conservative and minimally invasive approaches to control idiopathic condylar resorption: a scoping review[J]. Int J Oral Maxillofac Surg, 2023, 52(11): 1188-1196. |
| [27] | Gunson MJ, Arnett GW, Formby B, et al. Oral contraceptive pill use and abnormal menstrual cycles in women with severe condylar resorption: a case for low serum 17beta-estradiol as a major factor in progressive condylar resorption[J]. Am J Orthod Dentofacial Orthop, 2009, 136(6): 772-779. |
| [28] | Ye T, Sun DL, Mu T, et al. Differential effects of high-physiological oestrogen on the degeneration of mandibular condylar cartilage and subchondral bone[J]. Bone, 2018, 111: 9-22. |
| [29] | Park JH, Park JJ, Papademetriou M, et al. Anterior open bite due to idiopathic condylar resorption du-ring orthodontic retention of a Class Ⅱ Division 1 malocclusion[J]. Am J Orthod Dentofacial Orthop, 2019, 156(4): 555-565. |
| [30] | Ahmad N, Chen S, Wang W, et al. 17β-estradiol induces MMP-9 and MMP-13 in TMJ fibrochondrocytes via estrogen receptor α[J]. J Dent Res, 2018, 97(9): 1023-1030. |
| [31] | Iwasa A, Tanaka E. Signs, symptoms, and morphological features of idiopathic condylar resorption in orthodontic patients: a survey-based study[J]. J Clin Med, 2022, 11(6): 1552. |
| [32] | Robinson JL, Cass K, Aronson R, et al. Sex diffe-rences in the estrogen-dependent regulation of temporomandibular joint remodeling in altered loading[J]. Osteoarthritis Cartilage, 2017, 25(4): 533-543. |
| [33] | Choi J, Oh N, Kim IK. A follow-up study of condyle fracture in children[J]. Int J Oral Maxillofac Surg, 2005, 34(8): 851-858. |
| [34] | Lin YY, Tanaka N, Ohkuma S, et al. The mandibular cartilage metabolism is altered by damaged subchondral bone from traumatic impact loading[J]. Ann Biomed Eng, 2009, 37(7): 1358-1367. |
| [35] | Ji YD, Resnick CM, Peacock ZS. Idiopathic condylar resorption: a systematic review of etiology and management[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2020, 130(6): 632-639. |
| [36] | Barone S, Cosentini G, Bennardo F, et al. Incidence and management of condylar resorption after orthognathic surgery: an overview[J]. Korean J Orthod, 2022, 52(1): 29-41. |
| [37] | Nogami S, Yamauchi K, Satomi N, et al. Risk factors related to aggressive condylar resorption after orthognathic surgery for females: retrospective study[J]. Cranio, 2017, 35(4): 250-258. |
| [38] | Catherine Z, Breton P, Bouletreau P. Condylar resorption after orthognathic surgery: a systematic review[J]. Rev Stomatol Chir Maxillofac Chir Orale, 2016, 117(1): 3-10. |
| [39] | NiÑo-Sandoval TC, Almeida RAC, Vasconcelos BCDE. Incidence of condylar resorption after bimaxillary, LefortⅠ, and mandibular surgery: an overview[J]. Braz Oral Res, 2021, 35: e27. |
| [40] | de Moraes PH, Rizzati-Barbosa CM, Olate S, et al. Condylar resorption after orthognathic surgery: a systematic review[J]. Int J Morphol, 2012, 30(3): 1023-1028. |
| [41] | Mousoulea S, Kloukos D, Sampaziotis D, et al. Condylar resorption in orthognathic patients after mandibular bilateral sagittal split osteotomy: a systema-tic review[J]. Eur J Orthod, 2017, 39(3): 294-309. |
| [42] | Hwang SJ, Haers PE, Zimmermann A, et al. Surgical risk factors for condylar resorption after orthognathic surgery[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2000, 89(5): 542-552. |
| [43] | Scheerlinck JP, Stoelinga PJ, Blijdorp PA, et al. Sa-gittal split advancement osteotomies stabilized with miniplates. A 2-5-year follow-up[J]. Int J Oral Ma-xillofac Surg, 1994, 23(3): 127-131. |
| [44] | Yoshioka I, Khanal A, Tominaga K, et al. Vertical ramus versus sagittal split osteotomies: comparison of stability after mandibular setback[J]. J Oral Maxillofac Surg, 2008, 66(6): 1138-1144. |
| [45] | Kobayashi T, Izumi N, Kojima T, et al. Progressive condylar resorption after mandibular advancement[J]. Br J Oral Maxillofac Surg, 2012, 50(2): 176-180. |
| [46] | Nunes de Lima V, Faverani LP, Santiago JF, et al. Evaluation of condylar resorption rates after orthognathic surgery in Class Ⅱ and Ⅲ dentofacial deformities: a systematic review[J]. J Cranio Maxillofac Surg, 2018, 46(4): 668-673. |
| [47] | Vandeput AS, Verhelst PJ, Jacobs R, et al. Condylar changes after orthognathic surgery for Class Ⅲ dentofacial deformity: a systematic review[J]. Int J Oral Maxillofac Surg, 2019, 48(2): 193-202. |
| [48] | He Z, Ji HZ, Du W, et al. Management of condy-lar resorption before or after orthognathic surgery: a systematic review[J]. J Craniomaxillofac Surg, 2019, 47(7): 1007-1014. |
| [49] | Hoppenreijs TJ, Freihofer HP, Stoelinga PJ, et al. Condylar remodelling and resorption after Le Fort Ⅰand bimaxillary osteotomies in patients with anterior open bite. A clinical and radiological study[J]. Int J Oral Maxillofac Surg, 1998, 27(2): 81-91. |
| [50] | Park SB, Yang YM, Kim YI, et al. Effect of bimaxillary surgery on adaptive condylar head remodeling: metric analysis and image interpretation using cone-beam computed tomography volume superimposition[J]. J Oral Maxillofac Surg, 2012, 70(8): 1951-1959. |
| [51] | de Mol van Otterloo JJ, Dorenbos J, Tuinzing DB, et al. TMJ performance and behaviour in patients more than 6 years after Le FortⅠ osteotomy[J]. Br J Oral Maxillofac Surg, 1993, 31(2): 83-86. |
| [52] | Tanaka E, Koolstra JH. Biomechanics of the temporomandibular joint[J]. J Dent Res, 2008, 87(11): 989-991. |
| [53] | He YF, Lin H, Lin QP, et al. Morphologic changes in idiopathic condylar resorption with different degrees of bone loss[J]. Oral Surg Oral Med Oral Pa-thol Oral Radiol, 2019, 128(3): 332-340. |
| [54] | Alimanovic D, Pedersen TK, Matzen LH, et al. Comparing clinical and radiological manifestations of adolescent idiopathic condylar resorption and juvenile idiopathic arthritis in the temporomandibular joint[J]. J Oral Maxillofac Surg, 2021, 79(4): 774-785. |
| [55] | Cannizzaro E, Schroeder S, Bolt I, et al. Temporomandibular joint involvement in children with juvenile idiopathic arthritis[J]. Pediatr Rheumatol, 2008, 6(1): P92. |
| [56] | Boos-Lima FBDJ, Guastaldi FPS, Nielsen GP, et al. Histopathology of idiopathic condylar resorption differs from temporomandibular joint-only juvenile idiopathic arthritis[J]. J Oral Maxillofac Surg, 2025, 83(1): 26-36. |
| [57] | Shen P, Zhang D, Luo Y, et al. Characteristics of patients with temporomandibular joint idiopathic condylar resorption[J]. Cranio, 2025, 43(1): 151-157. |
| [58] | Raman P. Physiologic neuromuscular dental paradigm for the diagnosis and treatment of temporomandibular disorders[J]. J Calif Dent Assoc, 2014, 42(8): 563-571. |
| [59] | Papadaki ME, Tayebaty F, Kaban LB, et al. Condylar resorption[J]. Oral Maxillofac Surg Clin N Am, 2007, 19(2): 223-234. |
| [60] | Exposto CR, Stoustrup P, Kristensen KD, et al. Condylar changes in patients with idiopathic condylar resorption: retrospective 2-year follow-up CBCT-based case-control study[J]. Eur J Orthod, 2020, 42(6): 619-625. |
| [61] | Mao BC, Tian YJ, Li J, et al. A quantitative analysis of facial changes after orthodontic treatment with vertical control in patients with idiopathic condylar resorption[J]. Orthod Craniofac Res, 2023, 26(3): 402-414. |
| [62] | Yang HJ, Hwang SJ. Bone mineral density and mandibular advancement as contributing factors for postoperative relapse after orthognathic surgery in patients with preoperative idiopathic condylar resorption: a prospective study with preliminary 1-year follow-up[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2015, 120(2): 112-118. |
| [63] | Wang MJ, Qian YF, Zhao HJ, et al. Mandibular stability and condylar changes following orthognathic surgery in mandibular hypoplasia patients associa-ted with preoperative condylar resorption[J]. Clin Oral Investig, 2022, 26(12): 7083-7093. |
| [64] | Park Y, Chen S, Ahmad N, et al. Estrogen selectively enhances TMJ disc but not knee meniscus matrix loss[J]. J Dent Res, 2019, 98(13): 1532-1538. |
| [1] | 陈玉,雷银富,吴和梅,杜福兰,党洁,陈永梅,陶明,石兴莲. 口腔癌游离皮瓣重建患者气管切开术后肺炎风险预测模型的构建[J]. 国际口腔医学杂志, 2025, 52(5): 634-643. |
| [2] | 李榕,赵青. 基于颞下颌关节思考成人安氏Ⅱ2分类错 畸形的治疗[J]. 国际口腔医学杂志, 2024, 51(6): 687-698. |
| [3] | 李泽彬,刘鑫,王美青. 咬合与人体姿势关系的研究进展[J]. 国际口腔医学杂志, 2024, 51(6): 772-784. |
| [4] | 张桃李,龚衍吉,刘方,张秦兰蕙,刘洋. 颞下颌关节退行性改变与颅面形态及颞下颌关节形态结构的关联[J]. 国际口腔医学杂志, 2024, 51(5): 642-652. |
| [5] | 韩婧文,王蕾,任诗琦,王红宇,黄颖怡,李佳敏,郑艳. 青少年颞下颌关节形态特征与下颌骨三维方向生长的相关性研究[J]. 国际口腔医学杂志, 2024, 51(4): 456-466. |
| [6] | 张静,钟亦思,郑耘昊,张莉,熊鑫. 不同类型颞下颌关节紊乱病患者焦虑抑郁情绪的差异[J]. 国际口腔医学杂志, 2024, 51(3): 296-302. |
| [7] | 薛晴,齐慧川,胡敏. 机械应力下初级纤毛在骨和颞下颌关节软骨改建中力学感知作用的研究进展[J]. 国际口腔医学杂志, 2024, 51(2): 201-207. |
| [8] | 李沛然,毕瑞野,王旻,王瑞宇,刘尧,姜楠,曹品银,祝颂松. 上颌Le Fort Ⅰ前徙术与前份根尖下截骨后退术术后软组织变化的比较研究[J]. 国际口腔医学杂志, 2023, 50(3): 293-301. |
| [9] | 汪牡丹,宋东哲,黄定明. 开髓洞型对患牙根管治疗术后抗折性能影响的研究进展[J]. 国际口腔医学杂志, 2023, 50(2): 186-194. |
| [10] | 刘体倩,梁星,刘蔚晴,李晓虹,朱睿. 咬合创伤在牙周炎发生发展中的作用及机制的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 19-24. |
| [11] | 韩婧文,任诗琦,刘星宇,郎鑫,储梦诗,Waseem Saleh Abdo Kaid Algumaei,郑艳. 成人不同垂直及矢状骨面型髁突特征的研究[J]. 国际口腔医学杂志, 2022, 49(2): 153-162. |
| [12] | 李如意,罗锋,万乾炳. 下颌运动实时记录系统的原理及其应用进展[J]. 国际口腔医学杂志, 2022, 49(2): 182-189. |
| [13] | 杨赟琪,林阳阳,侯敏. 手术优先模式颌骨稳定性及影响因素研究进展[J]. 国际口腔医学杂志, 2022, 49(2): 227-232. |
| [14] | 张哲,刘进,王卫红,陈志强,杨春,刘丽. 焦磷酸钙沉积症继发颞下颌关节脱位1例[J]. 国际口腔医学杂志, 2021, 48(6): 664-667. |
| [15] | 许琳,王如意,勾薪瑞,王晓莉,李宇. 甲状旁腺激素相关蛋白调控下颌髁突软骨的研究进展[J]. 国际口腔医学杂志, 2021, 48(5): 549-555. |
|
||