国际口腔医学杂志 ›› 2019, Vol. 46 ›› Issue (5): 532-539.doi: 10.7518/gjkq.2019052
青薇1,黄丽娟1,郑佳俊1,任静1,李成龙2,庹嫱2,任小华3,牟雁东1,3( )
)
Qing Wei1,Huang Lijuan1,Zheng Jiajun1,Ren Jing1,Li Chenglong2,Tuo Qiang2,Ren Xiaohua3,Mu Yandong1,3()
摘要:
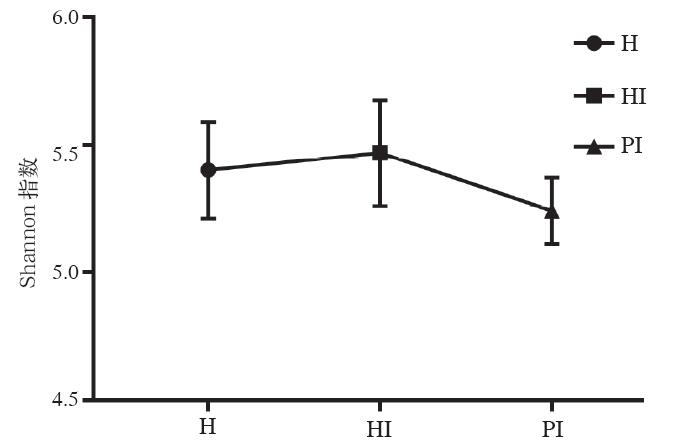
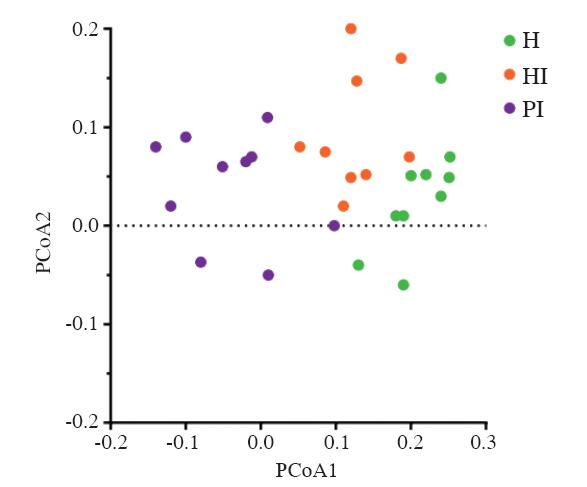
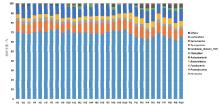
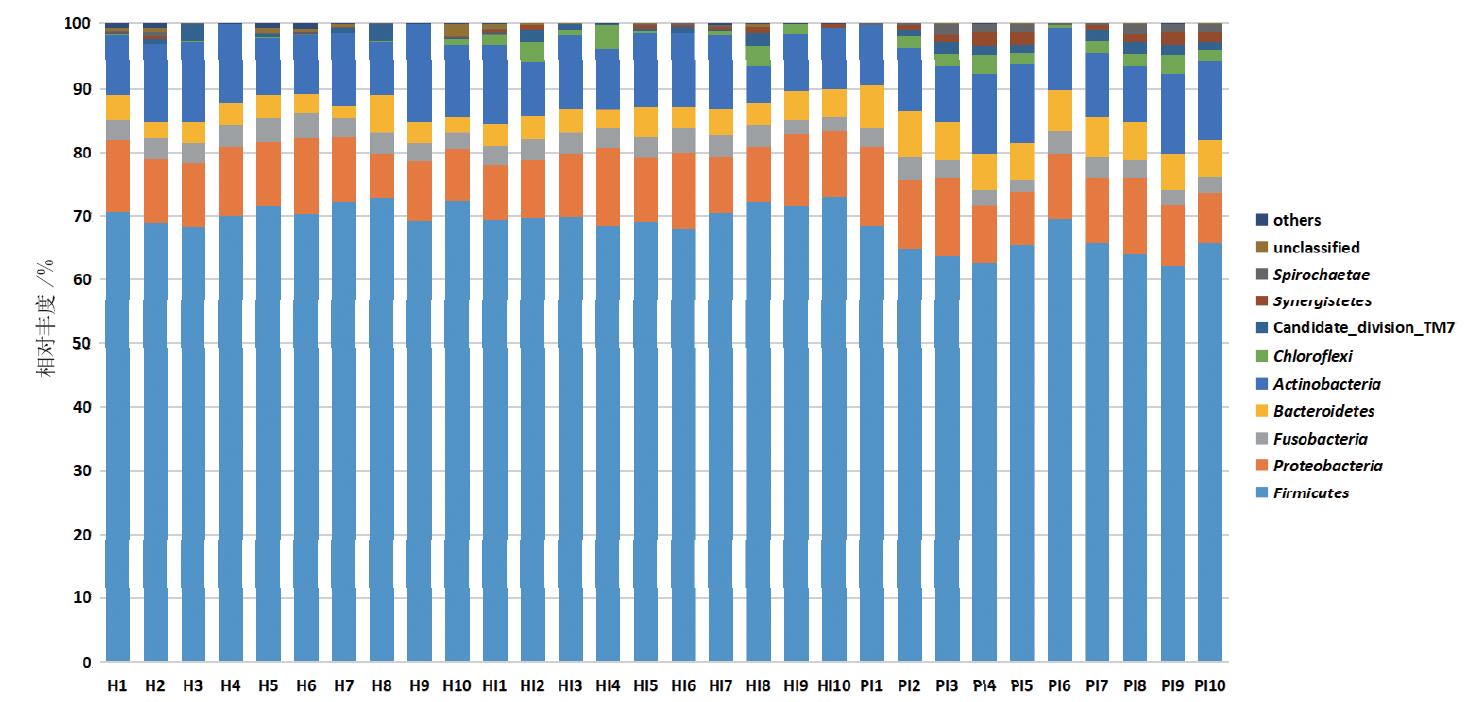
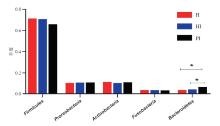
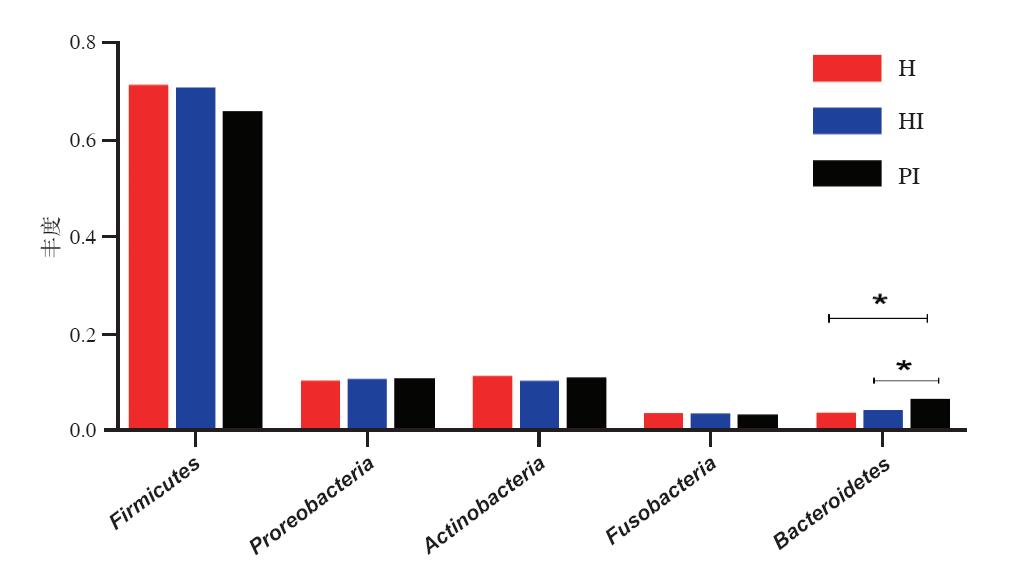
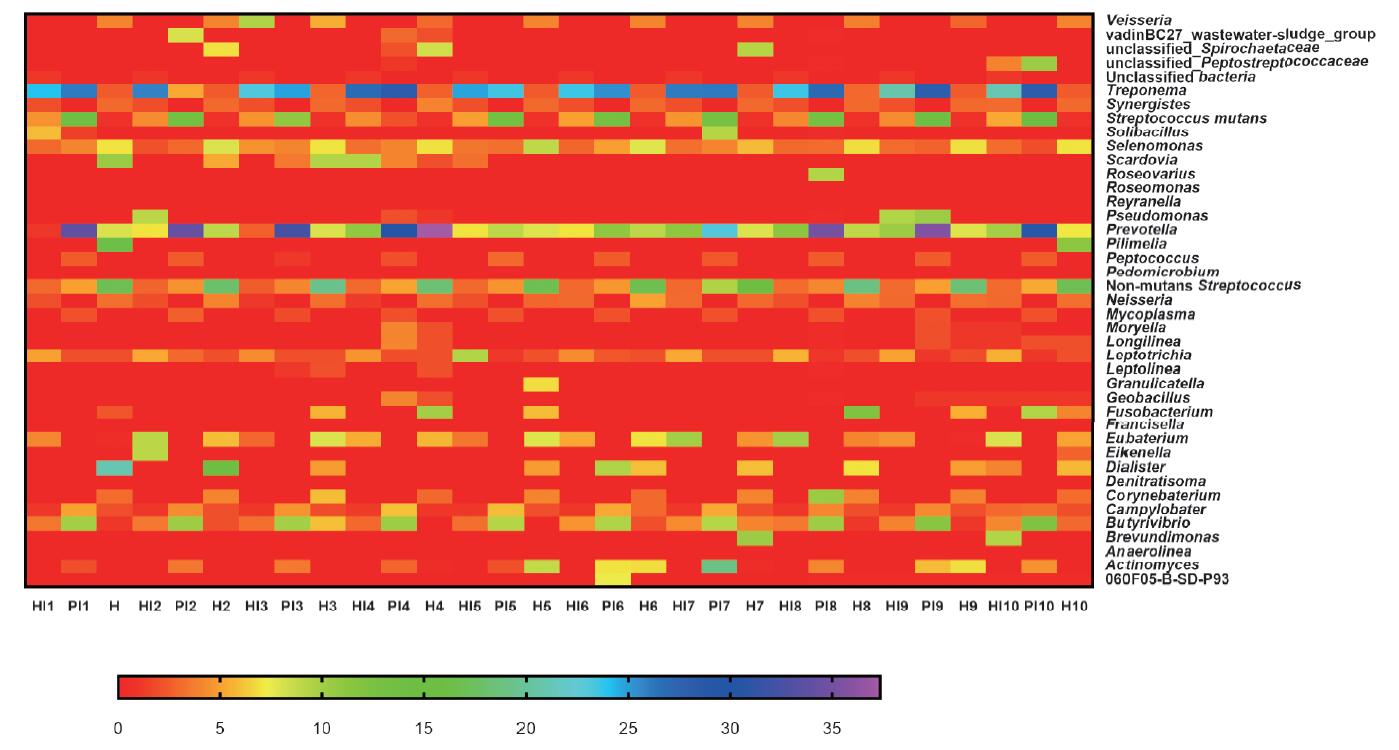
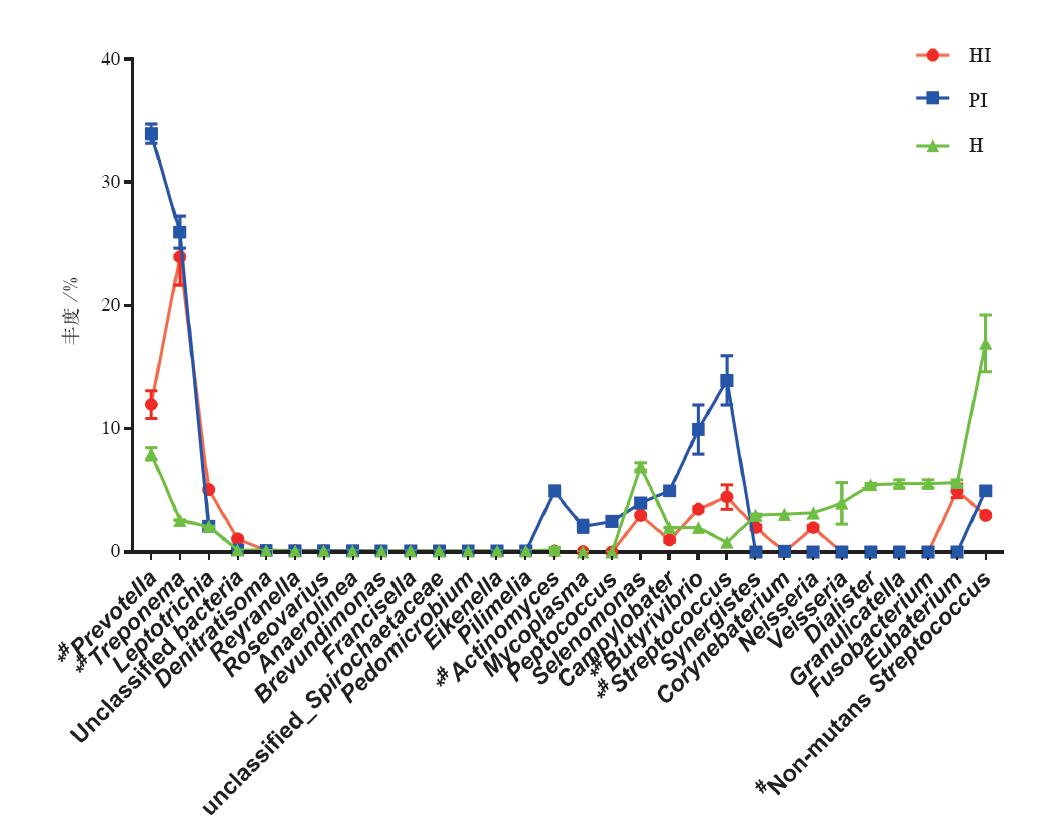
目的 应用16S核糖体DNA(rDNA)高通量测序技术研究健康天然牙、健康种植体以及种植体周围炎的植体龈沟液内微生物菌群的差异,为理解种植体周围组织从健康至疾病状态的病因提供依据。方法 通过Illumina HiSeq 2500测序技术,分析30个龈沟液细菌的菌群结构及多样性。结果 种植体周围炎组Shannon指数低于健康牙及健康种植体组(P<0.05),细菌群落主要属于厚壁菌门(Firmicutes)、变形菌门(Proteobacteria)、梭杆菌门(Fusobacteria)、拟杆菌门(Bacteroidetes)、放线菌门(Actinobacteria)等17个门,普氏菌属(Prevotella)、密螺旋体属(Treponema)、纤毛菌属(Leptotrichia)、放线菌属(Actinomyces)、链球菌属(Streptococcus)和丁酸弧菌属(Butyrivibrio)等497个属。优势菌门以拟杆菌门在种植体周围炎组相对较高(P<0.05),属水平上丁酸弧菌为种植体周围炎的优势菌属之一,代谢产物异丁酸的增多可能是导致疾病状态的一个因素。结论 健康种植体与健康天然牙一致,呈现出丰富的微生物多态性,而当周围炎形成后,表现为相关致病菌丰度增高,而其多样性下降。
中图分类号:
| [1] | Albrektsson T, Donos N , Working Group 1. Implant survival and complications. The Third EAO consen-sus conference 2012[J]. Clin Oral Implants Res, 2012,23(Suppl 6):63-65. |
| [2] | Mombelli A, Lang NP . The diagnosis and treatment of peri-implantitis[J]. Periodontol 2000, 1998,17:63-76. |
| [3] | Belibasakis GN . Microbiological and immuno-patho-logical aspects of peri-implant diseases[J]. Arch Oral Biol, 2014,59(1):66-72. |
| [4] | Renvert S, Quirynen M . Risk indicators for peri-im-plantitis. A narrative review[J]. Clin Oral Implants Res, 2015,26(Suppl 11):15-44. |
| [5] | Mombelli A, Müller N, Cionca N . The epidemiology of peri-implantitis[J]. Clin Oral Implants Res, 2012,23(Suppl 6):67-76. |
| [6] | 陈新, 熊萍, 钟科 , 等. 种植体周围黏膜炎龈下微生物群落多样性研究[J]. 口腔医学研究, 2015,31(7):719-723. |
| Chen X, Xiong P, Zhong K , et al. Study on the diversity of subgingival microflora in implant mucositis[J]. J Oral Sic Res, 2015,31(7):719-723. | |
| [7] | Wang T, Cai G, Qiu Y , et al. Structural segregation of gut microbiota between colorectal cancer patients and healthy volunteers[J]. ISME J, 2012,6(2):320-329. |
| [8] | 赵红, 王新林, 吕治 , 等. 基于高通量测序技术研究慢性牙周炎患者龈下刮治和根面平整术治疗前后龈下菌群的变化[J]. 国际口腔医学杂志, 2017,44(3):294-300. |
| Zhao H, Wang XL, Lü Z , et al. Microbiological community analysis by high-throughput sequencing of subgingival plaque in patients with chronic periodontitis before and after subgingival scaling and root planing[J]. Int J Stomatol, 2017,44(3):294-300. | |
| [9] | Persson GR, Renvert S . Cluster of bacteria associated with peri-implantitis[J]. Clin Implant Dent Relat Res, 2014,16(6):783-793. |
| [10] | Kumar PS, Mason MR, Brooker MR , et al. Pyrosequencing reveals unique microbial signatures as-sociated with healthy and failing dental implants[J]. J Clin Periodontol, 2012,39(5):425-433. |
| [11] | Al-Ahmad A, Muzafferiy F, Anderson AC , et al. Shift of microbial composition of peri-implantitis-associated oral biofilm as revealed by 16S rRNA gene cloning[J]. J Med Microbiol, 2018,67(3):332-340. |
| [12] | Edgar RC . UPARSE: highly accurate OTU sequences from microbial amplicon reads[J]. Nat Methods, 2013,10(10):996-998. |
| [13] | Kemp PF, Aller JY . Bacterial diversity in aquatic and other environments: what 16S rDNA libraries can tell us[J]. FEMS Microbiol Ecol, 2004,47(2):161-177. |
| [14] | Schwarz F, Derks J, Monje A , et al. Peri-implantitis[J]. J Periodontol, 2018,89(6):S267-S290. |
| [15] | Sorsa T, Hernández M, Leppilahti J , et al. Detection of gingival crevicular fluid MMP-8 levels with dif-ferent laboratory and chair-side methods[J]. Oral Dis, 2010,16(1):39-45. |
| [16] | Frey KG, Herrera-Galeano JE, Redden CL , et al. Comparison of three next-generation sequencing platforms for metagenomic sequencing and identi-fication of pathogens in blood[J]. BMC Genomics, 2014,15:96. |
| [17] | Koyanagi T, Sakamoto M, Takeuchi Y , et al. Compre-hensive microbiological findings in peri-implantitis and periodontitis[J]. J Clin Periodontol, 2013,40(3):218-226. |
| [18] |
吴芳, 李俊平, 汪珍珍 , 等. 16S rRNA基因克隆文库分析比较牙周炎患者和健康人口腔唾液微生物多样性[J]. 微生物学通报, 2016,43(6):1295-1303.
doi: 10.13344/j.microbiol.china.150792 |
|
Wu F, Li JP, Wang ZZ , et al. Comparison of oral microbial diversity between periodontitis patients and healthy people by 16S rRNA gene clone library[J]. Microbiolog, 2016,43(6):1295-1303.
doi: 10.13344/j.microbiol.china.150792 |
|
| [19] | Allen B, Kon M, Bar-Yam Y . A new phylogenetic diversity measure generalizing the Shannon index and its application to phyllostomid bats[J]. Am Nat, 2009,174(2):236-243. |
| [20] | Marsh PD . Microbial ecology of dental plaque and its significance in health and disease[J]. Adv Dent Res, 1994,8(2):263-271. |
| [21] | Kumar PS, Griffen AL, Moeschberger ML , et al. Identification of candidate periodontal pathogens and beneficial species by quantitative 16S clonal analysis[J]. J Clin Microbiol, 2005,43(8):3944-3955. |
| [22] | Preza D, Olsen I, Willumsen T , et al. Diversity and site-specificity of the oral microflora in the elderly[J]. Eur J Clin Microbiol Infect Dis, 2009,28(9):1033-1040. |
| [23] | Shibli JA, Melo L, Ferrari DS , et al. Composition of supra- and subgingival biofilm of subjects with heal-thy and diseased implants[J]. Clin Oral Implants Res, 2008,19(10):975-982. |
| [1] | 陆倩,夏海斌,王敏. 种植体磨光整形术治疗种植体周围炎的研究进展[J]. 国际口腔医学杂志, 2023, 50(2): 152-158. |
| [2] | 杨加震,张颖,刘育含,李帆,曾飞,李修珍,马玉莹,杨芳. 口腔诊疗环境细菌群落的时间变化趋势研究[J]. 国际口腔医学杂志, 2022, 49(2): 132-137. |
| [3] | 曹正国. 修复治疗相关的牙周问题考量[J]. 国际口腔医学杂志, 2022, 49(1): 1-11. |
| [4] | 郑桂婷,徐燕,吴明月. 种植体周围疾病治疗的专家共识及治疗方法的进展[J]. 国际口腔医学杂志, 2020, 47(6): 725-731. |
| [5] | 杨志雷,刘宝盈. 龋病牙菌斑微生态研究进展[J]. 国际口腔医学杂志, 2020, 47(5): 506-514. |
| [6] | 童子安,姒蜜思. 种植体表面菌斑去污方式的体外研究进展[J]. 国际口腔医学杂志, 2020, 47(5): 589-594. |
| [7] | 张敏,万浩元. 种植体周围炎药物治疗与激光治疗的研究进展[J]. 国际口腔医学杂志, 2020, 47(4): 463-470. |
| [8] | 吴秋月,李治邦. 药物辅助治疗种植体周围炎的研究进展[J]. 国际口腔医学杂志, 2020, 47(4): 471-477. |
| [9] | 黄海霞, 兰玉燕, 张昊, 潘兰兰, 郭玲, 刘敏. 慢性牙周炎患者种植修复后种植体牙周指数及龈沟液炎性因子水平的变化研究[J]. 国际口腔医学杂志, 2018, 45(4): 396-402. |
| [10] | 赵红, 王新林, 吕治, 王冬青, 苏建荣. 基于高通量测序技术研究慢性牙周炎患者龈下刮治和根面平整术治疗前后龈下菌群的变化[J]. 国际口腔医学杂志, 2017, 44(3): 294-300. |
| [11] | 孟令贤 班宇. 种植体表面去污联合手术疗法治疗种植体周围炎[J]. 国际口腔医学杂志, 2015, 42(4): 458-461. |
| [12] | 孙磊 夏荣. 钛基种植体表面抗菌改性的研究进展[J]. 国际口腔医学杂志, 2015, 42(4): 475-479. |
| [13] | 孙志新,张云涛. 口腔种植体周围炎与白细胞介素间的关系[J]. 国际口腔医学杂志, 2015, 42(2): 221-224. |
| [14] | 李允允 法永红. 透明质酸在口腔领域中的应用进展[J]. 国际口腔医学杂志, 2013, 40(3): 344-346. |
| [15] | 王柏翔综述 孟维艳审校. 种植体周围龈沟液检测分析的研究进展[J]. 国际口腔医学杂志, 2012, 39(6): 805-807. |
|