国际口腔医学杂志 ›› 2022, Vol. 49 ›› Issue (2): 132-137.doi: 10.7518/gjkq.2022017
杨加震1,2( ),张颖3,刘育含1,李帆4,曾飞1,2,李修珍1,马玉莹1,2,杨芳1()
),张颖3,刘育含1,李帆4,曾飞1,2,李修珍1,马玉莹1,2,杨芳1()
Yang Jiazhen1,2(),Zhang Ying3,Liu Yuhan1,Li Fan4,Zeng Fei1,2,Li Xiuzhen1,Ma Yuying1,2,Yang Fang1()
摘要:
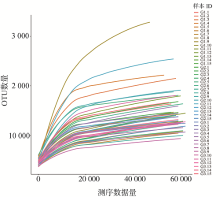
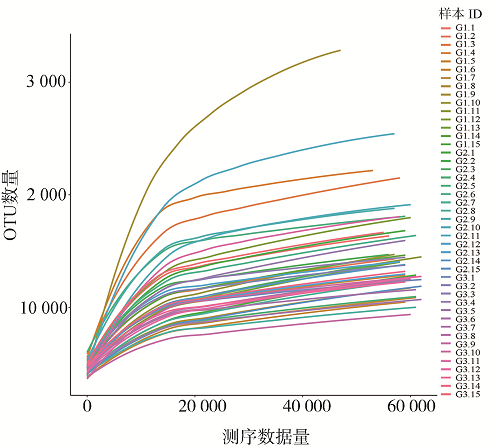
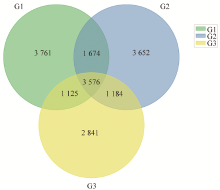
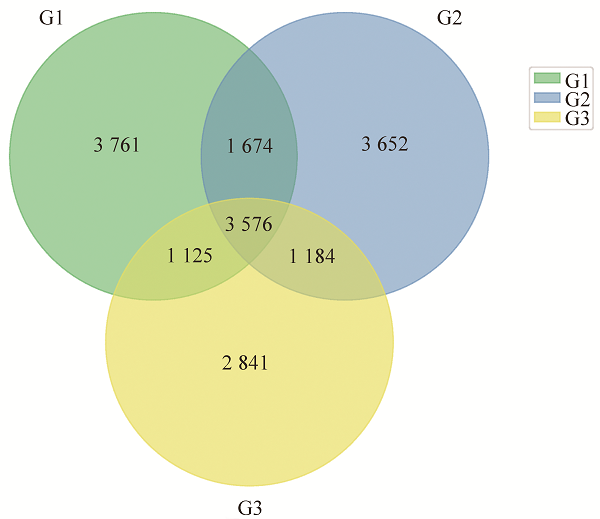
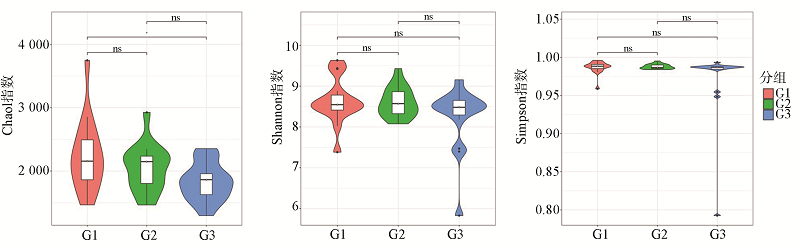
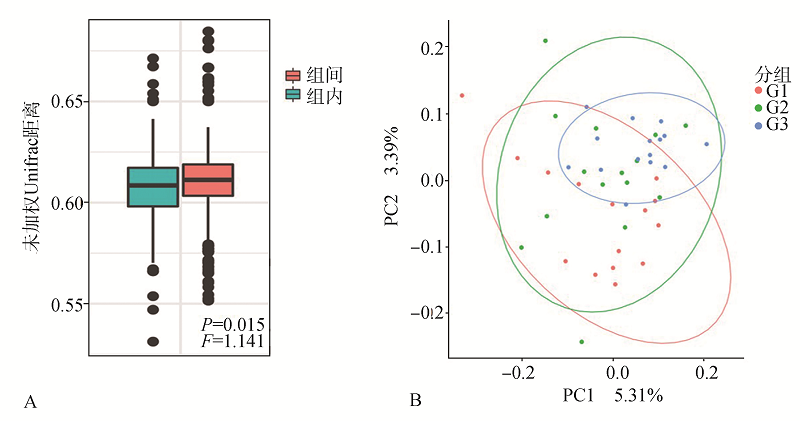
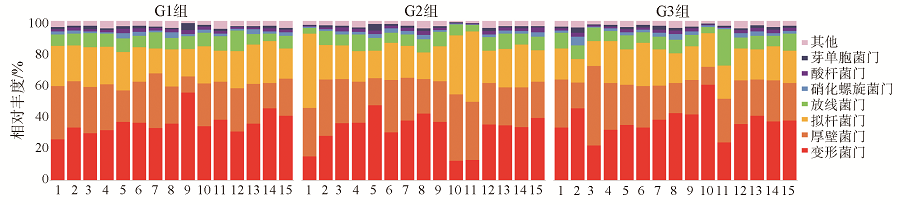
目的 应用16S rRNA高通量测序技术探究口腔诊疗环境细菌群落特征,及其随着投入使用时间增加的变化趋势,为口腔诊疗环境感染防控提供一定的理论依据。方法 选取新装修口腔内科诊室3间,分别于投入使用前(G1组)、使用1月(G2组)、使用3月(G3组),采集环境表面样本,利用Illumina MiSeq测序技术对16S rRNA V3-V4区测序,进行细菌群落结构及多样性差异分析。结果 G1组的物种丰富度高于G3组(P<0.05),3组间的菌落结构的差异具有统计学意义(P<0.05);细菌群落主要属于变形菌门、厚壁菌门、拟杆菌门等7个门,不同时间组的优势菌门占比相对稳定(P>0.05);丰度前30的细菌属中检测到埃希氏菌-志贺氏菌、链球菌、假单胞菌等7种潜在致病菌,其中埃希氏菌-志贺氏菌在诊室使用3月时明显增高(P<0.05),而假单胞菌明显降低(P<0.05)。结论 口腔诊疗环境呈现出丰富的细菌多样性,随着诊室投入使用周期延长,菌落结构更为相似。
中图分类号:
| [1] |
Mark Welch JL, Ramírez-Puebla ST, Borisy GG. Oral microbiome geography: micron-scale habitat and niche[J]. Cell Host Microbe, 2020, 28(2): 160-168.
doi: 10.1016/j.chom.2020.07.009 |
| [2] |
Rautemaa R, Nordberg A, Wuolijoki-Saaristo K, et al. Bacterial aerosols in dental practice-a potential hospital infection problem[J]. J Hosp Infect, 2006, 64(1): 76-81.
pmid: 16820249 |
| [3] |
Vidana R, Sillerström E, Ahlquist M, et al. Potential for nosocomial transmission of Enterococcus faecalis from surfaces in dental operatories[J]. Int Endod J, 2015, 48(6): 518-527.
doi: 10.1111/iej.12342 pmid: 25066305 |
| [4] |
Ricci ML, Fontana S, Pinci F, et al. Pneumonia associated with a dental unit waterline[J]. Lancet, 2012, 379(9816): 684.
doi: 10.1016/S0140-6736(12)60074-9 |
| [5] |
Boyce JM. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals[J]. Antimicrob Resist Infect Control, 2016, 5: 10.
doi: 10.1186/s13756-016-0111-x |
| [6] |
Stewart EJ. Growing unculturable bacteria[J]. J Bacteriol, 2012, 194(16): 4151-4160.
doi: 10.1128/JB.00345-12 pmid: 22661685 |
| [7] |
Merikanto I, Laakso JT, Kaitala V. Invasion ability and disease dynamics of environmentally growing opportunistic pathogens under outside-host competition[J]. PLoS One, 2014, 9(11): e113436.
doi: 10.1371/journal.pone.0113436 |
| [8] |
Zhang Y, Ping YF, Zhou RY, et al. High throughput sequencing-based analysis of microbial diversity in dental unit waterlines supports the importance of providing safe water for clinical use[J]. J Infect Public Health, 2018, 11(3): 357-363.
doi: 10.1016/j.jiph.2017.09.017 |
| [9] |
Costa D, Mercier A, Gravouil K, et al. Pyrosequencing analysis of bacterial diversity in dental unit waterlines[J]. Water Res, 2015, 81: 223-231.
doi: 10.1016/j.watres.2015.05.065 |
| [10] |
Rognes T, Flouri T, Nichols B, et al. VSEARCH: a versatile open source tool for metagenomics[J]. PeerJ, 2016, 4: e2584.
doi: 10.7717/peerj.2584 |
| [11] |
Caporaso JG, Kuczynski J, Stombaugh J, et al. QIIME allows analysis of high-throughput community sequencing data[J]. Nat Methods, 2010, 7(5): 335-336.
doi: 10.1038/nmeth.f.303 pmid: 20383131 |
| [12] |
Shobo CO, Alisoltani A, Abia ALK, et al. Bacterial diversity and functional profile of microbial populations on surfaces in public hospital environments in South Africa: a high throughput metagenomic analysis[J]. Sci Total Environ, 2020, 719: 137360.
doi: 10.1016/j.scitotenv.2020.137360 |
| [13] |
Chopyk J, Akrami K, Bavly T, et al. Temporal variations in bacterial community diversity and composition throughout intensive care unit renovations[J]. Microbiome, 2020, 8(1): 86.
doi: 10.1186/s40168-020-00852-7 |
| [14] | Rampelotto PH, Sereia AFR, de Oliveira LFV, et al. Exploring the hospital microbiome by high-resolution 16S rRNA profiling[J]. Int J Mol Sci, 2019, 20(12): E3099. |
| [15] |
Verma D, Garg PK, Dubey AK. Insights into the human oral microbiome[J]. Arch Microbiol, 2018, 200(4): 525-540.
doi: 10.1007/s00203-018-1505-3 |
| [16] |
Yu XL, Chan Y, Zhuang LF, et al. Intra-oral single-site comparisons of periodontal and peri-implant microbiota in health and disease[J]. Clin Oral Implants Res, 2019, 30(8): 760-776.
doi: 10.1111/clr.v30.8 |
| [17] |
Liu G, Wu C, Abrams WR, et al. Structural and functional characteristics of the microbiome in deep-dentin caries[J]. J Dent Res, 2020, 99(6): 713-720.
doi: 10.1177/0022034520913248 pmid: 32196394 |
| [18] |
Wang XW, Zhao ZB, Tang N, et al. Microbial community analysis of saliva and biopsies in patients with oral lichen planus[J]. Front Microbiol, 2020, 11: 629.
doi: 10.3389/fmicb.2020.00629 |
| [19] |
Xu J, Chen N, Wu Z, et al. 5-aminosalicylic acid alters the gut bacterial microbiota in patients with ulcerative colitis[J]. Front Microbiol, 2018, 9: 1274.
doi: 10.3389/fmicb.2018.01274 |
| [20] |
Fujitani S, Sun HY, Yu VL, et al. Pneumonia due to Pseudomonas aeruginosa: part Ⅰ: epidemiology, clinical diagnosis, and source[J]. Chest, 2011, 139(4): 909-919.
doi: S0012-3692(11)60194-3 pmid: 21467058 |
| [21] |
Mittal R, Aggarwal S, Sharma S, et al. Urinary tract infections caused by Pseudomonas aeruginosa: a minireview[J]. J Infect Public Health, 2009, 2(3): 101-111.
doi: 10.1016/j.jiph.2009.08.003 |
| [22] |
Wu DC, Chan WW, Metelitsa AI, et al. Pseudomonas skin infection: clinical features, epidemiology, and management[J]. Am J Clin Dermatol, 2011, 12(3): 157-169.
doi: 10.2165/11539770-000000000-00000 |
| [23] |
Willcox MD. Pseudomonas aeruginosa infection and inflammation during contact lens wear: a review[J]. Optom Vis Sci, 2007, 84(4): 273-278.
pmid: 17435510 |
| [24] |
Ribeiro LF, Lopes EM, Kishi LT, et al. Microbial community profiling in intensive care units expose limitations in current sanitary standards[J]. Front Public Health, 2019, 7: 240.
doi: 10.3389/fpubh.2019.00240 |
| [1] | 青薇,黄丽娟,郑佳俊,任静,李成龙,庹嫱,任小华,牟雁东. 16S核糖体DNA高通量测序研究种植体龈沟液微生物的变化[J]. 国际口腔医学杂志, 2019, 46(5): 532-539. |
| [2] | 赵红, 王新林, 吕治, 王冬青, 苏建荣. 基于高通量测序技术研究慢性牙周炎患者龈下刮治和根面平整术治疗前后龈下菌群的变化[J]. 国际口腔医学杂志, 2017, 44(3): 294-300. |
| [3] | 于淼 仪虹 郭笑. 母子间口腔群落结构的相关性分析[J]. 国际口腔医学杂志, 2015, 42(6): 664-667. |
| [4] | 蒙筱娴. 口腔综合治疗台在交叉感染中的媒体作用及控制[J]. 国际口腔医学杂志, 2000, 27(04): -. |
|