国际口腔医学杂志 ›› 2025, Vol. 52 ›› Issue (2): 217-230.doi: 10.7518/gjkq.2025020
曹昶1( ),张知妍1,何佳潞1,陈塑1,杨帆1,孟沙沙2,李岱蔚3,董永涛4,颜洁4,孙艳4,朱桂全1()
),张知妍1,何佳潞1,陈塑1,杨帆1,孟沙沙2,李岱蔚3,董永涛4,颜洁4,孙艳4,朱桂全1()
Chang Cao1(),Zhiyan Zhang1,Jialu He1,Su Chen1,Fan Yang1,Shasha Meng2,Daiwei Li3,Yongtao Dong4,Jie Yan4,Yan Sun4,Guiquan Zhu1()
摘要:
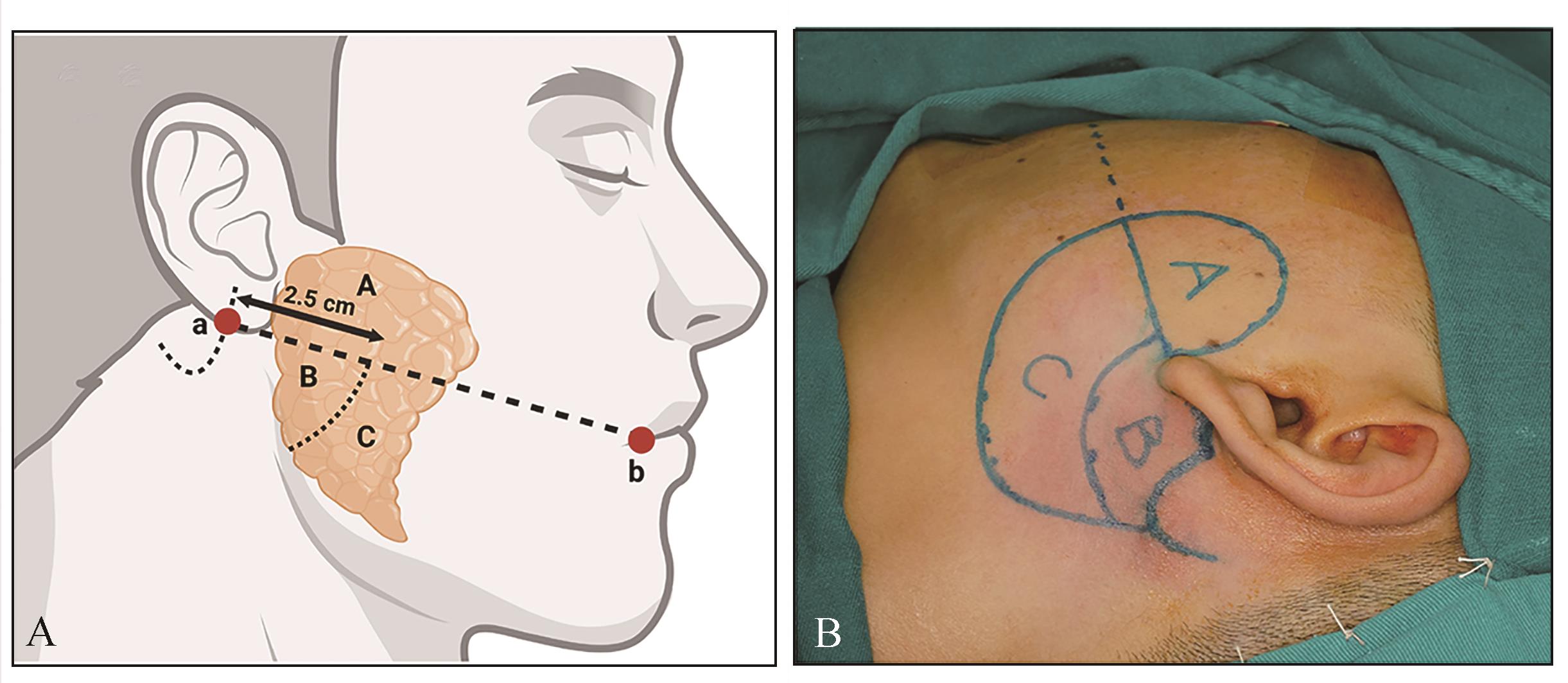
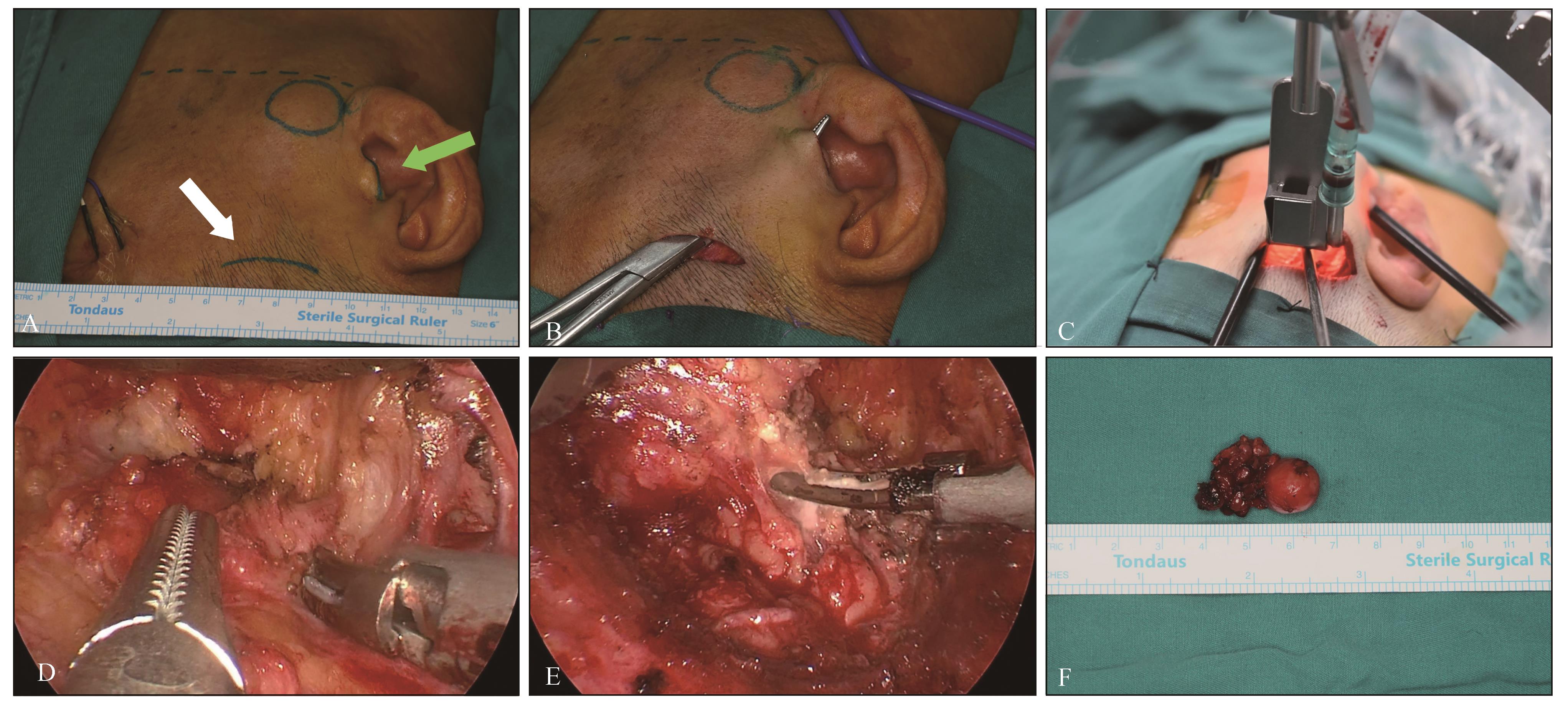
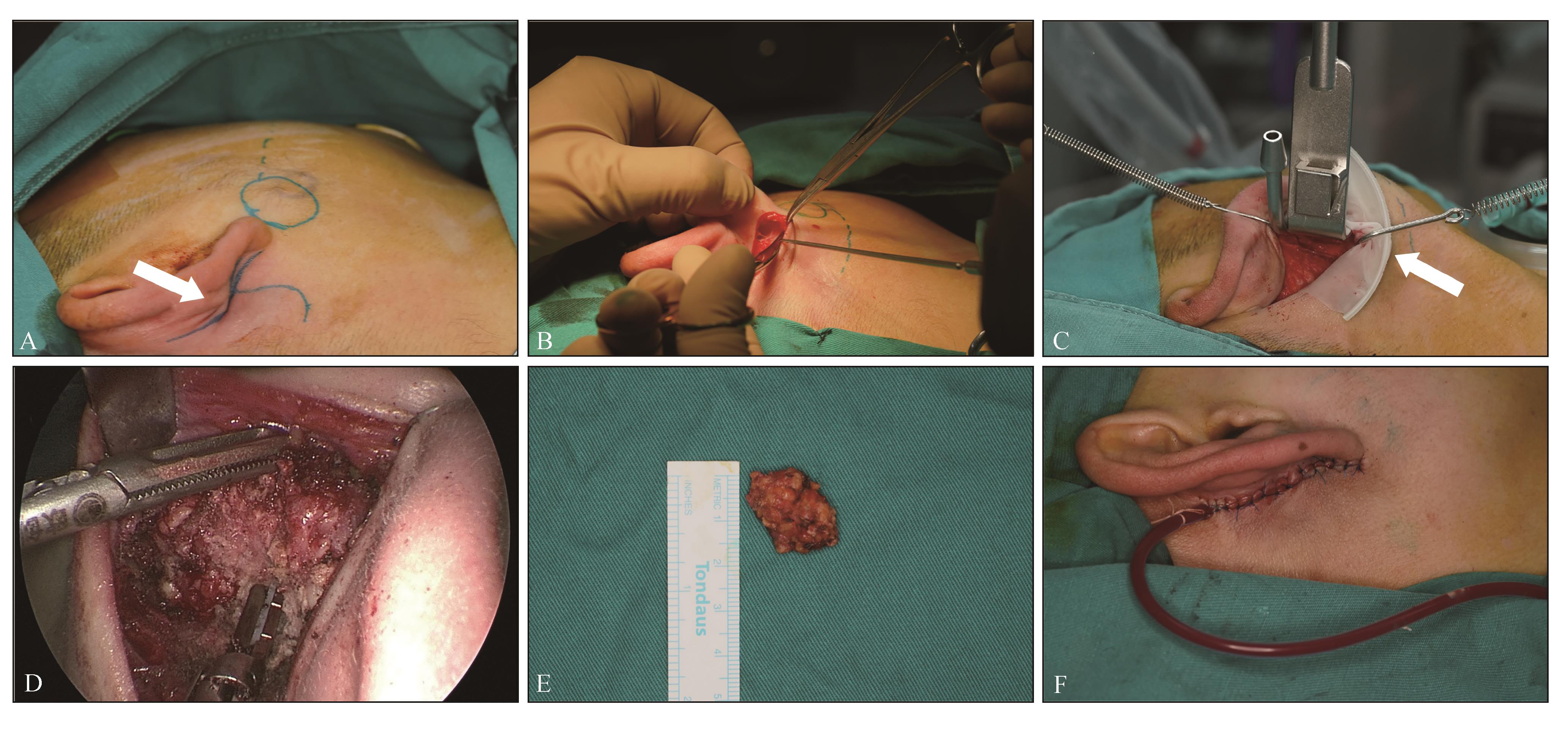
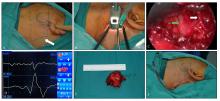
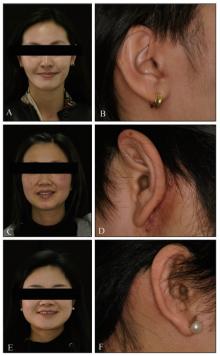
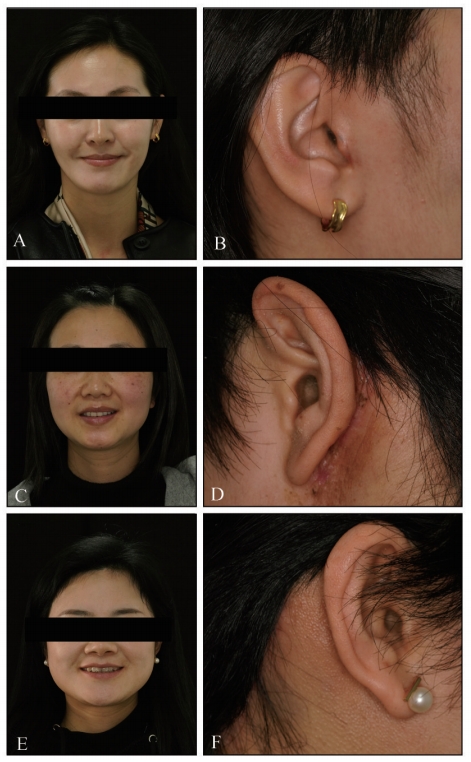
目的 评估一种基于ABC分区法的手术入路决策,在腮腺肿瘤内镜手术应用中的可行性、安全性及美观效果。 方法 回顾性纳入2022年1月1日—2024年1月1日于四川大学华西口腔医院头颈肿瘤外科接受免充气内镜下腮腺肿瘤切除术的95例患者。根据是否应用ABC分区法对患者进行分组,统计围手术期及随访数据。 结果 ABC分区法组患者的手术时间、术中出血量、术后引流量、涎瘘发生率、总住院时间均少于非分区法组,差异均有统计学意义(P<0.05)。非分区法组术后美观效果评价的视觉模拟评分为(1.63±0.88) 分,分区法组为(1.35±0.82)分,2组患者的差异无统计学意义(P>0.05),对术后美观效果均较为满意。 结论 采用ABC分区法匹配相应手术入路,可以提高腮腺肿瘤内镜手术的效率和微创性,加快术后康复,具有良好的安全性和美观效果。
中图分类号:
| 1 | Ungari C, Paparo F, Colangeli W, et al. Parotid glands tumours: overview of a 10-year experience with 282 patients, focusing on 231 benign epithelial neoplasms[J]. Eur Rev Med Pharmacol Sci, 2008, 12(5): 321-325. |
| 2 | Spiro RH. Salivary neoplasms: overview of a 35-year experience with 2, 807 patients[J]. Head Neck Surg, 1986, 8(3): 177-184. |
| 3 | Kim DY, Park GC, Cho YW, et al. Partial superficial parotidectomy via retroauricular hairline incision[J]. Clin Exp Otorhinolaryngol, 2014, 7(2): 119-122. |
| 4 | Huang XM, Zheng YQ, Liu X, et al. A comparison between endoscope-assisted partial parotidectomy and conventional partial parotidectomy[J]. Otolaryngol Head Neck Surg, 2009, 140(1): 70-75. |
| 5 | Chen WL, Fan S, Zhang DM. Endoscopically assis-ted extracapsular dissection of pleomorphic adenoma of the parotid gland through a postauricular sulcus approach in young patients[J]. Br J Oral Maxillofac Surg, 2017, 55(4): 400-403. |
| 6 | Fan S, Pan GK, Chen WL, et al. Endoscope-assisted extracapsular dissection of benign parotid tumors through a single cephaloauricular furrow incision versus a conventional approach[J]. Surg Endosc, 2017, 31(8): 3203-3209. |
| 7 | Moori PL, Rahman S. Endoscopic versus conventional parotid gland excision: a systematic review and meta-analysis[J]. Br J Oral Maxillofac Surg, 2021, 59(3): 272-280. |
| 8 | Lin SD, Tsai CC, Lai CS, et al. Endoscope-assisted parotidectomy for benign parotid tumors[J]. Ann Plast Surg, 2000, 45(3): 269-273. |
| 9 | Chen MK, Chang CC. Minimally invasive endoscope-assisted parotidectomy: a new approach[J]. Laryngoscope, 2007, 117(11): 1934-1937. |
| 10 | Chen JM, Chen WX, Zhang JL, et al. Modified endoscope-assisted partial-superficial parotidectomy through a retroauricular incision[J]. ORL J Otorhinolaryngol Relat Spec, 2014, 76(3): 121-126. |
| 11 | Gao L, Liang QL, Ren WH, et al. Comparison of endoscope-assisted versus conventional resection of parotid tumors[J]. Br J Oral Maxillofac Surg, 2019, 57(10): 1003-1008. |
| 12 | Chen S, Alkebsi K, Xuan M, et al. Single incision-plus approach for gasless endoscopic parotidectomy: a seven-step procedure[J]. Transl Cancer Res, 2022, 11(7): 2462-2472. |
| 13 | Woo SH, Kim JP, Baek CH. Endoscope-assisted extracapsular dissection of benign parotid tumors using hairline incision[J]. Head Neck, 2016, 38(3): 375-379. |
| 14 | Han P, Liang F, Lin P, et al. Comparison of conventional and endoscope-assisted partial superficial parotidectomy for benign neoplasms of the parotid gland: a matched case-control study[J]. Int J Oral Maxillofac Surg, 2024, 53(3): 199-204. |
| 15 | Zou HW, Gao J, Liu JX, et al. Feasibility and advantages of endoscope-assisted parotidectomy: a systematic review and meta-analysis[J]. Br J Oral Ma-xillofac Surg, 2021, 59(5): 503-510. |
| 16 | Yuan KF, Zhou B, Zhu CD, et al. Two-lines-four-regions: a new concept in endoscopic-assisted surgery of parotid gland tumors[J]. J Oral Maxillofac Surg, 2022, 80(7): 1284-1293. |
| 17 | 朱桂全, 李龙江. 内镜辅助的微创技术在口腔颌面外科中的历史、现状与展望[J]. 口腔颌面外科杂志, 2022, 32(5): 265-271. |
| Zhu GQ, Li LJ. History, current situation and prospects of the application of endoscope-assisted minimally invasive techniques in oral and maxillofacial surgery[J]. J Oral Maxillofac Surg, 2022, 32(5): 265-271. | |
| 18 | 朱桂全, 李春洁. 内镜下唾液腺切除术式的变迁与趋势——从内镜辅助到完全内镜[J]. 华西口腔医学杂志, 2023, 41(4): 377-384. |
| Zhu GQ, Li CJ. Developments and trends of endoscopic salivary gland resection: from endoscope-assisted to full endoscopic[J]. West China J Stomatol, 2023, 41(4): 377-384. | |
| 19 | Yang F, Alkebsi K, Chen S, et al. Gasless endosco-pic submandibular gland excision through hairline approach[J]. J Craniofac Surg, 2023, 34(5): 1563-1569. |
| 20 | 何佳潞, 陈塑, 杨帆, 等. 耳后发际入路完全腔镜下颌下腺切除术的临床分析[J]. 肿瘤预防与治疗, 2023, 36(11): 962-969. |
| He JL, Chen S, Yang F, et al. Full-endoscopic submandibular gland resection through retroauricular hairline approach: a clinical analysis[J]. J Cancer Contr Treat, 2023, 36(11): 962-969. | |
| 21 | 魏洪轩, 陈塑, 杨帆, 等. 耳后发际加颞部小切口入路免充气完全内镜下腮腺深叶肿瘤切除16例[J]. 中华口腔医学杂志, 2024, 59(2): 173-177. |
| Wei HX, Chen S, Yang F, et al. Postauricular hairline plus temporal approach gasless full-endoscopic parotidectomy for tumors in deep lobe of parotid gland: a 16-case report[J]. Chin J Stomatol, 2024, 59(2): 173-177. | |
| 22 | 杨帆, 曹昶, 孟莎莎, 等. 颈部无痕的舌癌颈淋巴清扫与游离皮瓣修复技术[J]. 实用口腔医学杂志, 2024, 40(1): 15-19. |
| Yang F, Cao C, Meng SS, et al. Neck dissection and free flap repair technique for tongue cancer without neck scar[J]. J Pract Stomatol, 2024, 40(1): 15-19. | |
| 23 | 朱桂全, 马中凯, 曹昶, 等. 国产手术机器人辅助下腮腺肿瘤切除1例[J]. 华西口腔医学杂志, 2024, 42(2): 262-267. |
| Zhu GQ, Ma ZK, Cao C, et al. Chinese surgical robot-assisted surgery for parotid tumor: a case report[J]. West China J Stomatol, 2024, 42(2): 262-267. | |
| 24 | Li TC, Liu YH, Wang QG, et al. Parotidectomy by an endoscopic-assisted postauricular-groove approa-ch[J]. Head Neck, 2019, 41(9): 2851-2859. |
| 25 | Hakim MA, McCain JP, Ahn DY, et al. Minimally invasive endoscopic oral and maxillofacial surgery[J]. Oral Maxillofac Surg Clin North Am, 2019, 31(4): 561-567. |
| 26 | 余佩武, 郝迎学. 中国西部地区微创外科发展现状与展望[J]. 中华胃肠外科杂志, 2017, 20(3): 244-246. |
| Yu PW, Hao YX. Development and future of minimally invasive surgery in Western China[J]. Chin J Gastrointest Surg, 2017, 20(3): 244-246. | |
| 27 | Koch M, Bozzato A, Iro H, et al. Combined endoscopic and transcutaneous approach for parotid gland sialolithiasis: indications, technique, and results[J]. Otolaryngol Head Neck Surg, 2010, 142(1): 98-103. |
| 28 | George KS, McGurk M. Extracapsular dissection: minimal resection for benign parotid tumours[J]. Br J Oral Maxillofac Surg, 2011, 49(6): 451-454. |
| 29 | 黄晓明, 郑亿庆, 孙伟, 等. 无注气内镜辅助下腮腺浅叶部分切除术[J]. 中华耳鼻咽喉头颈外科杂志, 2009, 44(6): 512-513. |
| Huang XM, Zheng YQ, Sun W, et al. Endoscope-assisted partial-superficial parotidectomy without CO2 infusion[J]. Chin J Otorhinolaryngol Head Neck Surg, 2009, 44(6): 512-513. | |
| 30 | 高力, 邵雁, 谢磊, 等. 隐蔽小切口内镜辅助下腮腺良性肿瘤切除术[J]. 中华整形外科杂志, 2004, 20(4): 290-293. |
| Gao L, Shao Y, Xie L, et al. Endoscope-assisted parotidectomy for benign tumors via a short hidden auricular incision[J]. Chin J Plast Surg, 2004, 20(4): 290-293. | |
| 31 | Zhao LD, Ye YS, Jiao JY, et al. Comparison of postoperative cytokine and hormone between endoscopically assisted and open parotid tumor resection[J]. Oral Dis, 2021, 27(7): 1720-1727. |
| 32 | 张志利, 邓璋, 魏宾, 等. 内镜辅助下腮腺浅叶良性肿瘤切除的临床应用[J]. 临床口腔医学杂志, 2022, 38(12): 734-737. |
| Zhang ZL, Deng Z, Wei B, et al. Clinical application of endoscope-assisted resection of benign paro-tid tumors in the superficial lobe of the parotid gland[J]. J Clin Stomatol, 2022, 38(12): 734-737. | |
| 33 | 李群星, 范松, 张汉卿, 等. 内镜辅助下经颅耳沟切口行腮腺良性肿瘤包膜外切除术[J]. 中华口腔医学研究杂志(电子版), 2016, 10(6): 408-413. |
| Li QX, Fan S, Zhang HQ, et al. Endoscope-assisted extracapsular dissection of benign parotid tumors through a single cephaloau-ricular furrow incision versus a conventional approach[J]. Chin J Stomatol Res (Electron Ed), 2016, 10(6): 408-413. | |
| 34 | 郑嫣然, 张凯. 内镜辅助下腮腺肿瘤手术和切口选择的研究进展[J]. 安徽医学, 2022, 43(10): 1234-1237. |
| Zheng YR, Zhang K. Research progress of endoscopic-assisted parotid tumor surgery and incision selection[J]. Anhui Med J, 2022, 43(10): 1234-1237. | |
| 35 | Iizuka K, Ishikawa K. Surgical techniques for benign parotid tumors: segmental resection vs extracapsular lumpectomy[J]. Acta Otolaryngol Suppl, 1998, 537: 75-81. |
| 36 | Gaillard C, Périé S, Susini B, et al. Facial nerve dysfunction after parotidectomy: the role of local factors[J]. Laryngoscope, 2005, 115(2): 287-291. |
| 37 | 冯铁军, 谢宇, 林雅琪, 等. 腔镜手术与传统手术对腮腺良性肿瘤的治疗效果的meta分析[J]. 南方医科大学学报, 2021, 41(3): 464-470. |
| Feng TJ, Xie Y, Lin YQ, et al. Comparison of endoscopic versus conventional surgery for benign paro-tid tumor: a meta analysis[J]. J South Med Univ, 2021, 41(3): 464-470. |
| [1] | 揭伟萍,胡济安,李怡宁. 唾液腺微分泌性腺癌临床病理的研究进展[J]. 国际口腔医学杂志, 2025, 52(2): 257-262. |
| [2] | 沈洁,何地,刘雁鸣. 下颌下腺良性肿瘤功能性手术的研究进展[J]. 国际口腔医学杂志, 2021, 48(2): 230-237. |
|