Int J Stomatol ›› 2025, Vol. 52 ›› Issue (2): 217-230.doi: 10.7518/gjkq.2025020
• Original Articles • Previous Articles Next Articles
Chang Cao1( ),Zhiyan Zhang1,Jialu He1,Su Chen1,Fan Yang1,Shasha Meng2,Daiwei Li3,Yongtao Dong4,Jie Yan4,Yan Sun4,Guiquan Zhu1()
),Zhiyan Zhang1,Jialu He1,Su Chen1,Fan Yang1,Shasha Meng2,Daiwei Li3,Yongtao Dong4,Jie Yan4,Yan Sun4,Guiquan Zhu1()
CLC Number:
| 1 | Ungari C, Paparo F, Colangeli W, et al. Parotid glands tumours: overview of a 10-year experience with 282 patients, focusing on 231 benign epithelial neoplasms[J]. Eur Rev Med Pharmacol Sci, 2008, 12(5): 321-325. |
| 2 | Spiro RH. Salivary neoplasms: overview of a 35-year experience with 2, 807 patients[J]. Head Neck Surg, 1986, 8(3): 177-184. |
| 3 | Kim DY, Park GC, Cho YW, et al. Partial superficial parotidectomy via retroauricular hairline incision[J]. Clin Exp Otorhinolaryngol, 2014, 7(2): 119-122. |
| 4 | Huang XM, Zheng YQ, Liu X, et al. A comparison between endoscope-assisted partial parotidectomy and conventional partial parotidectomy[J]. Otolaryngol Head Neck Surg, 2009, 140(1): 70-75. |
| 5 | Chen WL, Fan S, Zhang DM. Endoscopically assis-ted extracapsular dissection of pleomorphic adenoma of the parotid gland through a postauricular sulcus approach in young patients[J]. Br J Oral Maxillofac Surg, 2017, 55(4): 400-403. |
| 6 | Fan S, Pan GK, Chen WL, et al. Endoscope-assisted extracapsular dissection of benign parotid tumors through a single cephaloauricular furrow incision versus a conventional approach[J]. Surg Endosc, 2017, 31(8): 3203-3209. |
| 7 | Moori PL, Rahman S. Endoscopic versus conventional parotid gland excision: a systematic review and meta-analysis[J]. Br J Oral Maxillofac Surg, 2021, 59(3): 272-280. |
| 8 | Lin SD, Tsai CC, Lai CS, et al. Endoscope-assisted parotidectomy for benign parotid tumors[J]. Ann Plast Surg, 2000, 45(3): 269-273. |
| 9 | Chen MK, Chang CC. Minimally invasive endoscope-assisted parotidectomy: a new approach[J]. Laryngoscope, 2007, 117(11): 1934-1937. |
| 10 | Chen JM, Chen WX, Zhang JL, et al. Modified endoscope-assisted partial-superficial parotidectomy through a retroauricular incision[J]. ORL J Otorhinolaryngol Relat Spec, 2014, 76(3): 121-126. |
| 11 | Gao L, Liang QL, Ren WH, et al. Comparison of endoscope-assisted versus conventional resection of parotid tumors[J]. Br J Oral Maxillofac Surg, 2019, 57(10): 1003-1008. |
| 12 | Chen S, Alkebsi K, Xuan M, et al. Single incision-plus approach for gasless endoscopic parotidectomy: a seven-step procedure[J]. Transl Cancer Res, 2022, 11(7): 2462-2472. |
| 13 | Woo SH, Kim JP, Baek CH. Endoscope-assisted extracapsular dissection of benign parotid tumors using hairline incision[J]. Head Neck, 2016, 38(3): 375-379. |
| 14 | Han P, Liang F, Lin P, et al. Comparison of conventional and endoscope-assisted partial superficial parotidectomy for benign neoplasms of the parotid gland: a matched case-control study[J]. Int J Oral Maxillofac Surg, 2024, 53(3): 199-204. |
| 15 | Zou HW, Gao J, Liu JX, et al. Feasibility and advantages of endoscope-assisted parotidectomy: a systematic review and meta-analysis[J]. Br J Oral Ma-xillofac Surg, 2021, 59(5): 503-510. |
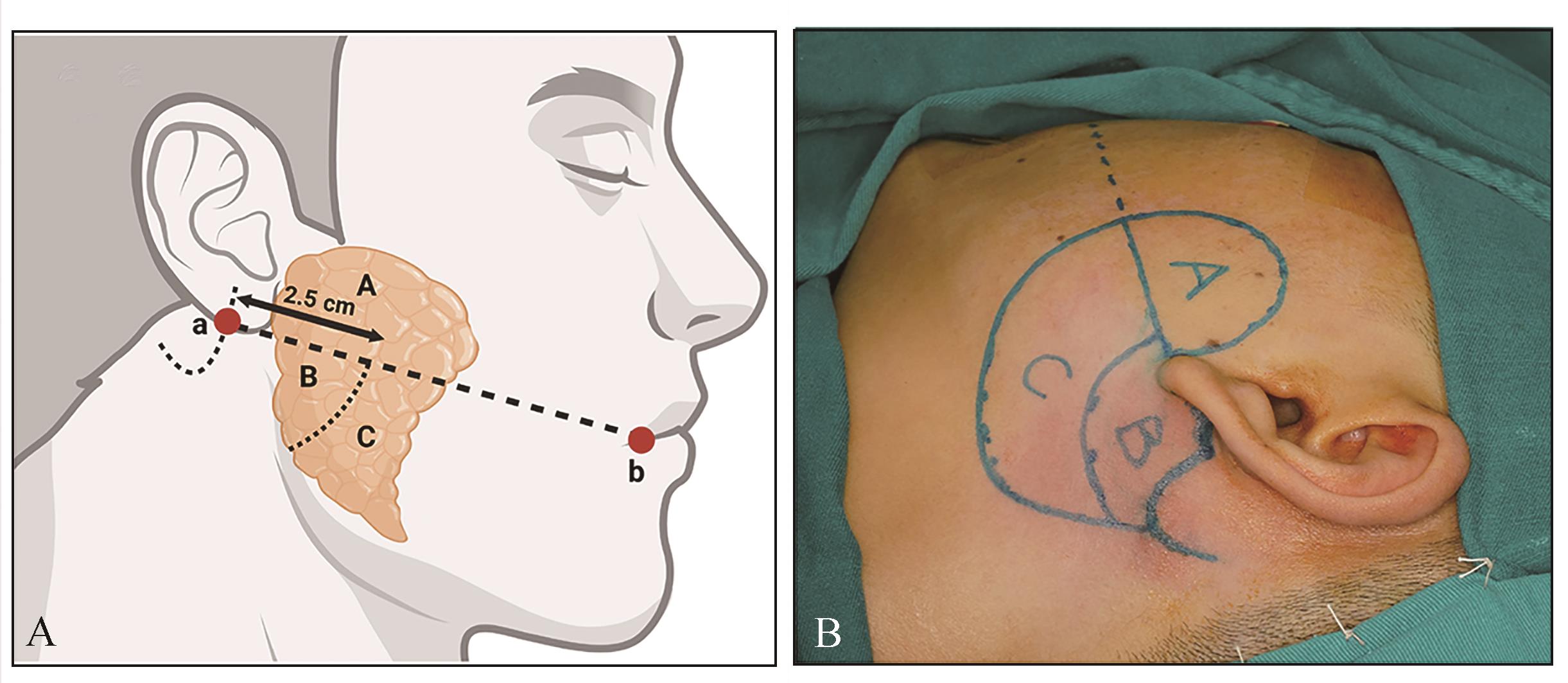
| 16 | Yuan KF, Zhou B, Zhu CD, et al. Two-lines-four-regions: a new concept in endoscopic-assisted surgery of parotid gland tumors[J]. J Oral Maxillofac Surg, 2022, 80(7): 1284-1293. |
| 17 | 朱桂全, 李龙江. 内镜辅助的微创技术在口腔颌面外科中的历史、现状与展望[J]. 口腔颌面外科杂志, 2022, 32(5): 265-271. |
| Zhu GQ, Li LJ. History, current situation and prospects of the application of endoscope-assisted minimally invasive techniques in oral and maxillofacial surgery[J]. J Oral Maxillofac Surg, 2022, 32(5): 265-271. | |
| 18 | 朱桂全, 李春洁. 内镜下唾液腺切除术式的变迁与趋势——从内镜辅助到完全内镜[J]. 华西口腔医学杂志, 2023, 41(4): 377-384. |
| Zhu GQ, Li CJ. Developments and trends of endoscopic salivary gland resection: from endoscope-assisted to full endoscopic[J]. West China J Stomatol, 2023, 41(4): 377-384. | |
| 19 | Yang F, Alkebsi K, Chen S, et al. Gasless endosco-pic submandibular gland excision through hairline approach[J]. J Craniofac Surg, 2023, 34(5): 1563-1569. |
| 20 | 何佳潞, 陈塑, 杨帆, 等. 耳后发际入路完全腔镜下颌下腺切除术的临床分析[J]. 肿瘤预防与治疗, 2023, 36(11): 962-969. |
| He JL, Chen S, Yang F, et al. Full-endoscopic submandibular gland resection through retroauricular hairline approach: a clinical analysis[J]. J Cancer Contr Treat, 2023, 36(11): 962-969. | |
| 21 | 魏洪轩, 陈塑, 杨帆, 等. 耳后发际加颞部小切口入路免充气完全内镜下腮腺深叶肿瘤切除16例[J]. 中华口腔医学杂志, 2024, 59(2): 173-177. |
| Wei HX, Chen S, Yang F, et al. Postauricular hairline plus temporal approach gasless full-endoscopic parotidectomy for tumors in deep lobe of parotid gland: a 16-case report[J]. Chin J Stomatol, 2024, 59(2): 173-177. | |
| 22 | 杨帆, 曹昶, 孟莎莎, 等. 颈部无痕的舌癌颈淋巴清扫与游离皮瓣修复技术[J]. 实用口腔医学杂志, 2024, 40(1): 15-19. |
| Yang F, Cao C, Meng SS, et al. Neck dissection and free flap repair technique for tongue cancer without neck scar[J]. J Pract Stomatol, 2024, 40(1): 15-19. | |
| 23 | 朱桂全, 马中凯, 曹昶, 等. 国产手术机器人辅助下腮腺肿瘤切除1例[J]. 华西口腔医学杂志, 2024, 42(2): 262-267. |
| Zhu GQ, Ma ZK, Cao C, et al. Chinese surgical robot-assisted surgery for parotid tumor: a case report[J]. West China J Stomatol, 2024, 42(2): 262-267. | |
| 24 | Li TC, Liu YH, Wang QG, et al. Parotidectomy by an endoscopic-assisted postauricular-groove approa-ch[J]. Head Neck, 2019, 41(9): 2851-2859. |
| 25 | Hakim MA, McCain JP, Ahn DY, et al. Minimally invasive endoscopic oral and maxillofacial surgery[J]. Oral Maxillofac Surg Clin North Am, 2019, 31(4): 561-567. |
| 26 | 余佩武, 郝迎学. 中国西部地区微创外科发展现状与展望[J]. 中华胃肠外科杂志, 2017, 20(3): 244-246. |
| Yu PW, Hao YX. Development and future of minimally invasive surgery in Western China[J]. Chin J Gastrointest Surg, 2017, 20(3): 244-246. | |
| 27 | Koch M, Bozzato A, Iro H, et al. Combined endoscopic and transcutaneous approach for parotid gland sialolithiasis: indications, technique, and results[J]. Otolaryngol Head Neck Surg, 2010, 142(1): 98-103. |
| 28 | George KS, McGurk M. Extracapsular dissection: minimal resection for benign parotid tumours[J]. Br J Oral Maxillofac Surg, 2011, 49(6): 451-454. |
| 29 | 黄晓明, 郑亿庆, 孙伟, 等. 无注气内镜辅助下腮腺浅叶部分切除术[J]. 中华耳鼻咽喉头颈外科杂志, 2009, 44(6): 512-513. |
| Huang XM, Zheng YQ, Sun W, et al. Endoscope-assisted partial-superficial parotidectomy without CO2 infusion[J]. Chin J Otorhinolaryngol Head Neck Surg, 2009, 44(6): 512-513. | |
| 30 | 高力, 邵雁, 谢磊, 等. 隐蔽小切口内镜辅助下腮腺良性肿瘤切除术[J]. 中华整形外科杂志, 2004, 20(4): 290-293. |
| Gao L, Shao Y, Xie L, et al. Endoscope-assisted parotidectomy for benign tumors via a short hidden auricular incision[J]. Chin J Plast Surg, 2004, 20(4): 290-293. | |
| 31 | Zhao LD, Ye YS, Jiao JY, et al. Comparison of postoperative cytokine and hormone between endoscopically assisted and open parotid tumor resection[J]. Oral Dis, 2021, 27(7): 1720-1727. |
| 32 | 张志利, 邓璋, 魏宾, 等. 内镜辅助下腮腺浅叶良性肿瘤切除的临床应用[J]. 临床口腔医学杂志, 2022, 38(12): 734-737. |
| Zhang ZL, Deng Z, Wei B, et al. Clinical application of endoscope-assisted resection of benign paro-tid tumors in the superficial lobe of the parotid gland[J]. J Clin Stomatol, 2022, 38(12): 734-737. | |
| 33 | 李群星, 范松, 张汉卿, 等. 内镜辅助下经颅耳沟切口行腮腺良性肿瘤包膜外切除术[J]. 中华口腔医学研究杂志(电子版), 2016, 10(6): 408-413. |
| Li QX, Fan S, Zhang HQ, et al. Endoscope-assisted extracapsular dissection of benign parotid tumors through a single cephaloau-ricular furrow incision versus a conventional approach[J]. Chin J Stomatol Res (Electron Ed), 2016, 10(6): 408-413. | |
| 34 | 郑嫣然, 张凯. 内镜辅助下腮腺肿瘤手术和切口选择的研究进展[J]. 安徽医学, 2022, 43(10): 1234-1237. |
| Zheng YR, Zhang K. Research progress of endoscopic-assisted parotid tumor surgery and incision selection[J]. Anhui Med J, 2022, 43(10): 1234-1237. | |
| 35 | Iizuka K, Ishikawa K. Surgical techniques for benign parotid tumors: segmental resection vs extracapsular lumpectomy[J]. Acta Otolaryngol Suppl, 1998, 537: 75-81. |
| 36 | Gaillard C, Périé S, Susini B, et al. Facial nerve dysfunction after parotidectomy: the role of local factors[J]. Laryngoscope, 2005, 115(2): 287-291. |
| 37 | 冯铁军, 谢宇, 林雅琪, 等. 腔镜手术与传统手术对腮腺良性肿瘤的治疗效果的meta分析[J]. 南方医科大学学报, 2021, 41(3): 464-470. |
| Feng TJ, Xie Y, Lin YQ, et al. Comparison of endoscopic versus conventional surgery for benign paro-tid tumor: a meta analysis[J]. J South Med Univ, 2021, 41(3): 464-470. |
| [1] | Weiping Jie,Ji’an Hu,Yining Li. Clinical pathological study on the microsecretory adenocarcinoma of salivary glands [J]. Int J Stomatol, 2025, 52(2): 257-262. |
| [2] | Shen Jie,He Di,Liu Yanming. Research progress on the functional surgery of benign submandibular gland tumors [J]. Int J Stomatol, 2021, 48(2): 230-237. |