国际口腔医学杂志 ›› 2026, Vol. 53 ›› Issue (4): 476-486.doi: 10.7518/gjkq.2026226
夏寒萍1( ),刘娟1,肖闻澜2,姚毓洁1,童昕2,闫福华1,陈斌1()
),刘娟1,肖闻澜2,姚毓洁1,童昕2,闫福华1,陈斌1()
Hanping Xia1(),Juan Liu1,Wenlan Xiao2,Yujie Yao1,Xin Tong2,Fuhua Yan1,Bin Chen1()
摘要:
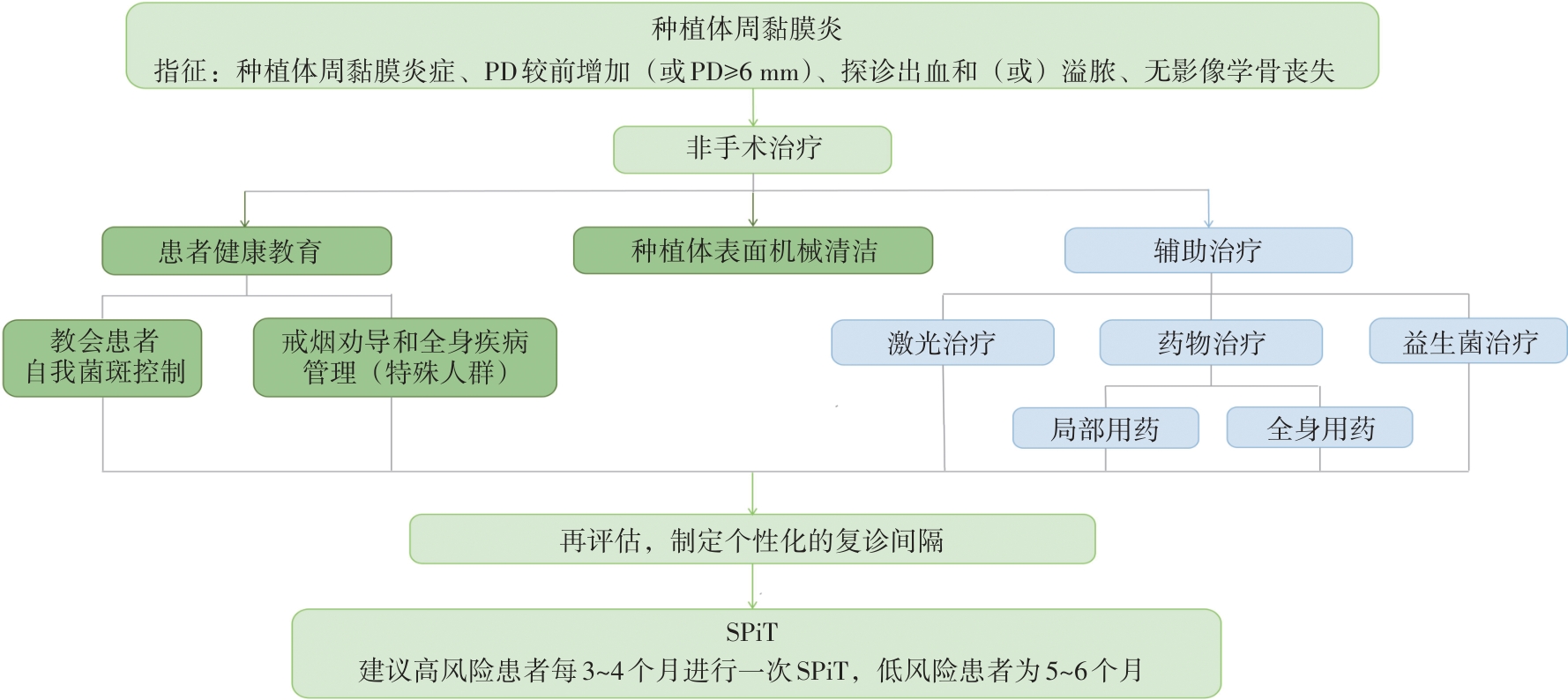
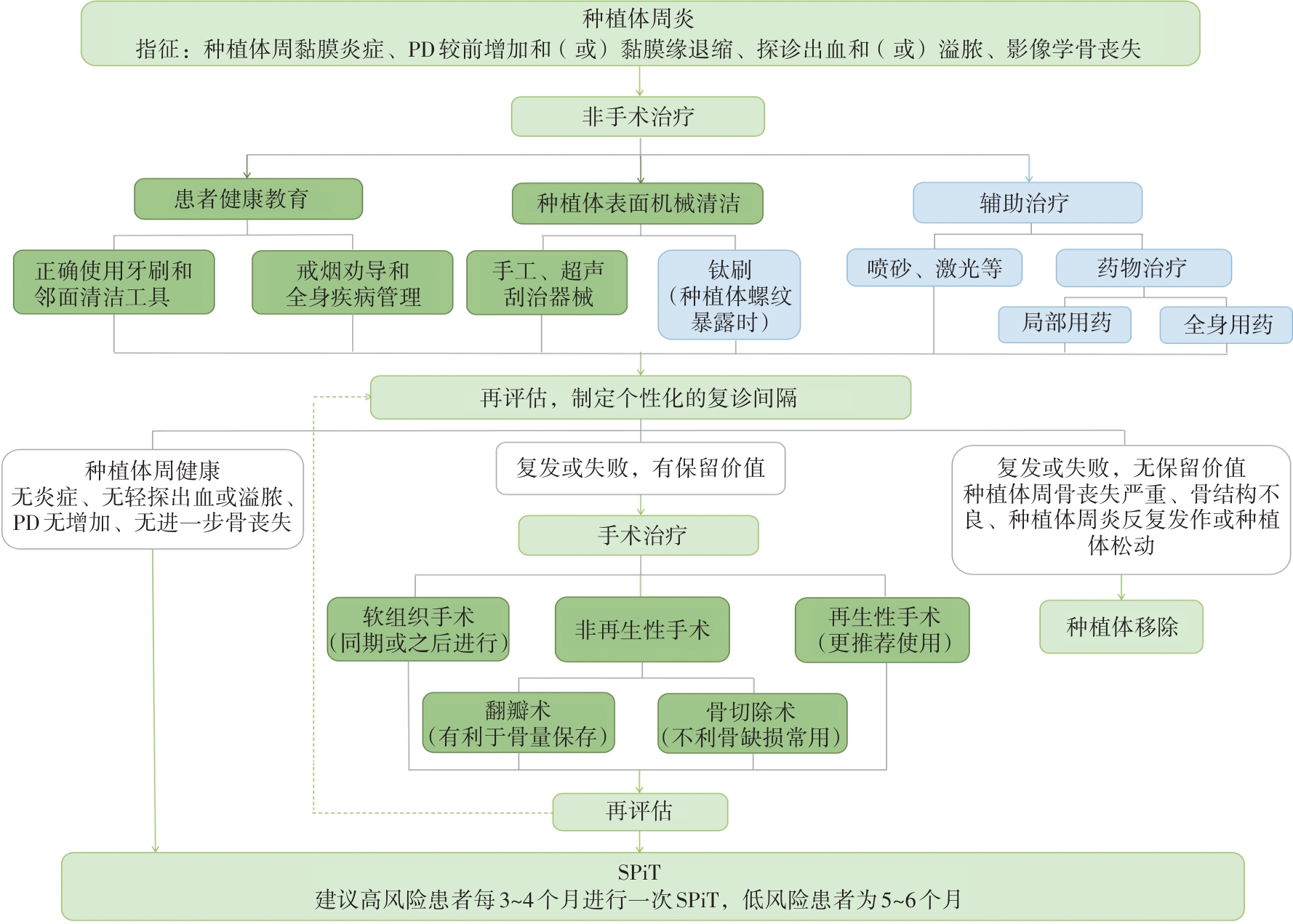
2025年6月骨整合学会和美国牙周病学会联合制定的关于预防和管理种植体周病和状况的专家共识发布,该共识基于8篇系统评价,重点关注种植体周黏膜炎、种植体周炎、种植体周软组织缺损以及种植体周边缘骨丧失的危险因素和防治策略,分析了全身疾病、行为因素、患者因素、种植位点局部条件、手术因素和修复设计等对种植体周病和状况发生的影响并对其风险程度进行分级,随后基于这些风险因素对不同种植体周病和状况的防治提出了指导意见。本文拟结合我国国情对该共识进行要点解读,梳理循证医学证据和专家共识意见,以提高国内医生对种植体周病和状况防治的理解,从而提高种植体留存率。
中图分类号:
| [1] | Kim WJ, Cho YD, Ku Y, et al. The worldwide pa-tent landscape of dental implant technology[J]. Biomater Res, 2022, 26(1): 59. |
| [2] | Herrera D, Sanz M, Kebschull M, et al. Treatment of stage Ⅳ periodontitis: the EFP S3 level clinical practice guideline[J]. J Clin Periodontol, 2022, 49(): 4-71. |
| [3] | West N, Chapple I, Culshaw S, et al. BSP Implementation of prevention and treatment of peri-implant diseases—the EFP S3 level clinical practice guideline[J]. J Dent, 2024, 149: 104980. |
| [4] | Wang HL, Avila-Ortiz G, Monje A, et al. AO/AAP consensus on prevention and management of peri-implant diseases and conditions: summary report[J]. J Periodontol, 2025, 96(6): 519-541. |
| [5] | Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology[J]. J Clin Periodontol, 2015, 42(): S158-S171. |
| [6] | Lee CT, Huang YW, Zhu L, et al. Prevalences of peri-implantitis and peri-implant mucositis: systema-tic review and meta-analysis[J]. J Dent, 2017, 62: 1-12. |
| [7] | Romandini M, Lima C, Pedrinaci I, et al. Prevalence and risk/protective indicators of peri-implant disea-ses: a university-representative cross-sectional study[J]. Clin Oral Implants Res, 2021, 32(1): 112-122. |
| [8] | Apaza-Bedoya K, Galarraga-Vinueza ME, Correa BB, et al. Prevalence, risk indicators, and clinical characteristics of peri-implant mucositis and peri-implantitis for an internal conical connection implant system: a multicenter cross-sectional study[J]. J Periodontol, 2024, 95(6): 582-593. |
| [9] | Obreja K, Ramanauskaite A, Begic A, et al. The prevalence of peri-implant diseases around subcres-tally placed implants: a cross-sectional study[J]. Clin Oral Implants Res, 2021, 32(6): 702-710. |
| [10] | Shi JY, Jie N, Zhuang LF, et al. Peri-implant conditions and marginal bone loss around cemented and screw-retained single implant crowns in posterior regions: a retrospective cohort study with up to 4 years follow-up[J]. PLoS One, 2018, 13(2): e0191717. |
| [11] | Tavelli L, Barootchi S. Prevalence, incidence, risk, and protective factors for soft tissue dehiscences at implant sites in the absence of disease: an AO/AAP systematic review and meta-regression analysis[J]. J Periodontol, 2025, 96(6): 562-586. |
| [12] | Gamborena I, Avila-Ortiz G. Peri-implant marginal mucosa defects: classification and clinical management[J]. J Periodontol, 2021, 92(7): 947-957. |
| [13] | Romandini M, Pedrinaci I, Lima C, et al. Prevalence and risk/protective indicators of buccal soft tissue dehiscence around dental implants[J]. J Clin Periodontol, 2021, 48(3): 455-463. |
| [14] | Renvert S, Polyzois I. Treatment of pathologic peri-implant pockets[J]. Periodontol 2000, 2018, 76(1): 180-190. |
| [15] | Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review[J]. Int J Oral Maxillofac Implants, 2014, 29(): 325-345. |
| [16] | Sanz M, Solonko M, Luengo F. Key factors in prevention of peri-implant diseases[J]. Compend Contin Educ Dent, 2017, 38(8 ): 6-13. |
| [17] | Carra MC, Blanc-Sylvestre N, Courtet A, et al. Primordial and primary prevention of peri-implant di-seases: a systematic review and meta-analysis[J]. J Clin Periodontol, 2023, 50(): 77-112. |
| [18] | Lee JCY, Mattheos N, Nixon KC, et al. Residual periodontal pockets are a risk indicator for peri-implantitis in patients treated for periodontitis[J]. Clin Oral Implants Res, 2012, 23(3): 325-333. |
| [19] | Roccuzzo A, Imber JC, Marruganti C, et al. Clinical outcomes of dental implants in patients with and without history of periodontitis: a 20-year prospective study[J]. J Clin Periodontol, 2022, 49(12): 1346-1356. |
| [20] | Alhakeem M, Kanounisabet N, Nowzari H, et al. Risk indicators of long-term outcome of implant therapy in patients with a history of severe periodontitis or no history of periodontitis: a retrospective cohort study[J]. Int J Dent Hyg, 2023, 21(1): 227-237. |
| [21] | Renvert S, Polyzois I. Risk indicators for peri-implant mucositis: a systematic literature review[J]. J Clin Periodontol, 2015, 42(): S172-S186. |
| [22] | Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review[J]. Clin Oral Implants Res, 2015, 26(): 15-44. |
| [23] | Costa FO, Lages EJP, Cortelli SC, et al. Association between cumulative smoking exposure, span since smoking cessation, and peri-implantitis: a cross-sectional study[J]. Clin Oral Investig, 2022, 26(7): 4835-4846. |
| [24] | Galindo-Moreno P, Fauri M, Avila-Ortiz G, et al. Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study[J]. Clin Oral Implants Res, 2005, 16(5): 579-586. |
| [25] | Carr BR, Boggess WJ, Coburn JF, et al. Does alcohol consumption protect against late dental implant failures[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2021, 131(6): 631-637. |
| [26] | Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis[J]. J Dent Res, 2016, 95(4): 372-379. |
| [27] | Chan D, Pelekos G, Ho D, et al. The depth of the implant mucosal tunnel modifies the development and resolution of experimental peri-implant mucositis: a case-control study[J]. J Clin Periodontol, 2019, 46(2): 248-255. |
| [28] | Monje A, Kan JY, Borgnakke W. Impact of local predisposing/precipitating factors and systemic dri-vers on peri-implant diseases[J]. Clin Implant Dent Relat Res, 2023, 25(4): 640-660. |
| [29] | Galindo-Moreno P, León-Cano A, Ortega-Oller I, et al. Prosthetic abutment height is a key factor in peri-implant marginal bone loss[J]. J Dent Res, 2014, 93(7 ): 80S-85S. |
| [30] | Blanco J, Pico A, Caneiro L, et al. Effect of abutment height on interproximal implant bone level in the early healing: a randomized clinical trial[J]. Clin Oral Implants Res, 2018, 29(1): 108-117. |
| [31] | Katafuchi M, Weinstein BF, Leroux BG, et al. Restoration contour is a risk indicator for peri-implantitis: a cross-sectional radiographic analysis[J]. J Clin Periodontol, 2018, 45(2): 225-232. |
| [32] | Strauss FJ, Siegenthaler M, Hämmerle CHF, et al. Restorative angle of zirconia restorations cemented on non-original titanium bases influences the initial marginal bone loss: 5-year results of a prospective cohort study[J]. Clin Oral Implants Res, 2022, 33(7): 745-756. |
| [33] | Mattheos N, Janda M, Acharya A, et al. Impact of design elements of the implant supracrestal complex (ISC) on the risk of peri-implant mucositis and peri-implantitis: a critical review[J]. Clin Oral Implants Res, 2021, 32(): 181-202. |
| [34] | Pjetursson BE, Thoma D, Jung R, et al. A systema-tic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years[J]. Clin Oral Implants Res, 2012, 23(): 22-38. |
| [35] | Zucchelli G, Tavelli L, Stefanini M, et al. Classification of facial peri-implant soft tissue dehiscence/deficiencies at single implant sites in the esthetic zone[J]. J Periodontol, 2019, 90(10): 1116-1124. |
| [36] | Kumar PS, Kan J, Galarraga-Vinueza ME, et al. Risk for peri-implant diseases and defects: report of workgroup 1 of the joint AO/AAP consensus confe-rence on prevention and management of peri-implant diseases[J]. Clin Adv Periodontics, 2025, 15(2): 93-102. |
| [37] | Fiorellini JP, Mojaver S, Sarmiento H, et al. Clinical translation of the 2024 AO/AAP consensus on prevention and management of peri-implant diseases and conditions[J]. Int J Periodontics Restorative Dent, 2025, 45(4): 1-23. |
| [38] | Galarraga-Vinueza ME, Pagni S, Finkelman M, et al. Prevalence, incidence, systemic, behavioral, and patient-related risk factors and indicators for peri-implant diseases: an AO/AAP systematic review and meta-analysis[J]. J Periodontol, 2025, 96(6): 587-633. |
| [39] | Monje A, Barootchi S, Rosen PS, et al. Surgical- and implant-related factors and onset/progression of peri-implant diseases: an AO/AAP systematic review[J]. J Periodontol, 2025, 96(6): 542-561. |
| [40] | Lin GH, Lee E, Barootchi S, et al. The influence of prosthetic designs on peri-implant bone loss: an AO/AAP systematic review and meta-analysis[J]. J Pe-riodontol, 2025, 96(6): 634-651. |
| [41] | Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Di-seases and Conditions[J]. J Clin Periodontol, 2018, 45(): S286-S291. |
| [42] | Tavelli L, Barootchi S, Majzoub J, et al. Volumetric changes at implant sites: a systematic appraisal of traditional methods and optical scanning-based digital technologies[J]. J Clin Periodontol, 2021, 48(2): 315-334. |
| [43] | Tavelli L, Barootchi S, Majzoub J, et al. Prevalence and risk indicators of midfacial peri-implant soft tissue dehiscence at single site in the esthetic zone: a cross-sectional clinical and ultrasonographic study[J]. J Periodontol, 2022, 93(6): 857-866. |
| [44] | Sanz-Martín I, Regidor E, Navarro J, et al. Factors associated with the presence of peri-implant buccal soft tissue dehiscences: a case-control study[J]. J Periodontol, 2020, 91(8): 1003-1010. |
| [45] | Lin GH, Chambrone L, Rajendran Y, et al. Treatment of peri-implant mucositis: an AAP/AO syste-matic review and meta-analysis[J]. Int J Oral Maxillofac Implants, 2025(4): 49-72. |
| [46] | Ravidà A, Dias DR, Lemke R, et al. Efficacy of decontamination methods for biofilm removal from dental implant surfaces and reosseointegration: an AAP/AO systematic review on peri-implant disea-ses and conditions[J]. Int J Oral Maxillofac Implants, 2025(4): 91-160. |
| [47] | Saleh MHA, Misch C, Alrmali A, et al. Efficacy of nonreconstructive surgical treatment of peri-implantitis: an AAP/AO systematic review and meta-analysis of access flap versus osseous surgery procedures[J]. Int J Oral Maxillofac Implants, 2025(4): 73-90. |
| [48] | Barootchi S, Monje A, Sabri H, et al. Surgical reconstructive therapy for the management of peri-implantitis: an AAP/AO systematic review and network meta-analysis[J]. Int J Oral Maxillofac Implants, 2025(4): 1-48. |
| [49] | Figuero E, Graziani F, Sanz I, et al. Management of peri-implant mucositis and peri-implantitis[J]. Perio-dontol 2000, 2014, 66(1): 255-273. |
| [50] | Jepsen S, Berglundh T, Genco R, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis[J]. J Clin Periodontol, 2015, 42(): S152-S157. |
| [51] | Rakic M, Tatic Z, Radovanovic S, et al. Resolution of peri-implant mucositis following standard treatment: a prospective split-mouth study[J]. J Perio-dontol, 2024, 95(9): 842-852. |
| [52] | Iorio-Siciliano V, Blasi A, Isola G, et al. Resolution of peri-implant mucositis at tissue- and bone-level implants: a 6-month prospective controlled clinical trial[J]. Clin Oral Implants Res, 2023, 34(5): 450- 462. |
| [53] | Herrera D, Berglundh T, Schwarz F, et al. Prevention and treatment of peri-implant diseases—the EFP S3 level clinical practice guideline[J]. J Clin Periodontol, 2023, 50(): 4-76. |
| [54] | Roccuzzo M, Layton DM, Roccuzzo A, et al. Clinical outcomes of peri-implantitis treatment and supportive care: a systematic review[J]. Clin Oral Implants Res, 2018, 29(): 331-350. |
| [55] | Butera A, Maiorani C, Gallo S, et al. Evaluation of adjuvant systems in non-surgical peri-implant treatment: a literature review[J]. Healthcare, 2022, 10(5): 886. |
| [56] | Blanco C, Pico A, Dopico J, et al. Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. A randomized placebo-controlled clinical trial[J]. J Clin Periodontol, 2022, 49(1): 15-27. |
| [57] | Ramanauskaite A, Schwarz F. Current concepts for the treatment of peri-implant disease[J]. Int J Pros-thodont, 2024, 37(2): 124-134. |
| [58] | Schwarz F, John G, Mainusch S, et al. Combined surgical therapy of peri-implantitis evaluating two methods of surface debridement and decontamination. A two-year clinical follow up report[J]. J Clin Periodontol, 2012, 39(8): 789-797. |
| [59] | Monje A, Pons R, Peña P. Electrolytic surface decontamination in the reconstructive therapy of peri-implantitis: single-center outcomes[J]. Int J Perio-dontics Restorative Dent, 2025, 45(2): 185-198. |
| [60] | Carcuac O, Derks J, Abrahamsson I, et al. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial[J]. J Clin Perio-dontol, 2017, 44(12): 1294-1303. |
| [61] | Karlsson K, Derks J, Håkansson J, et al. Interventions for peri-implantitis and their effects on further bone loss: a retrospective analysis of a registry-based cohort[J]. J Clin Periodontol, 2019, 46(8): 872-879. |
| [62] | Donos N, Calciolari E, Ghuman M, et al. The efficacy of bone reconstructive therapies in the management of peri-implantitis. A systematic review and meta-analysis[J]. J Clin Periodontol, 2023, 50(): 285-316. |
| [1] | 夏溦瑶,王婧,屈依丽. 逆行性种植体周炎病因与治疗的研究进展[J]. 国际口腔医学杂志, 2026, 53(4): 496-502. |
| [2] | 李佳敏,李毓晨,葛张洁,廖凌子,郭鑫,郭晓龙,周平. 抗菌肽在口腔钛种植体涂层中的研究进展[J]. 国际口腔医学杂志, 2024, 51(5): 572-584. |
| [3] | 满毅, 黄定明. 美学区种植骨增量与邻牙慢性根尖周病的联合治疗策略(上):应用基础及适应证[J]. 国际口腔医学杂志, 2022, 49(5): 497-505. |
|