国际口腔医学杂志 ›› 2020, Vol. 47 ›› Issue (2): 166-174.doi: 10.7518/gjkq.2020051
薛伶俐,李雅冬( )
)
Xue Lingli,Li Yadong()
摘要:
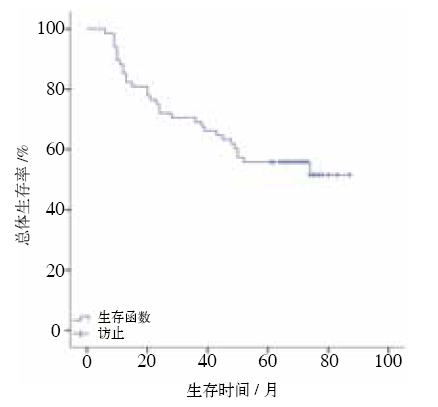
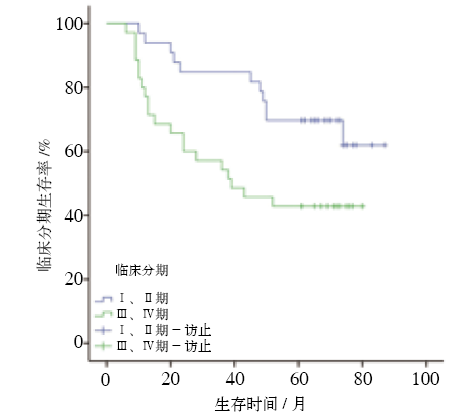
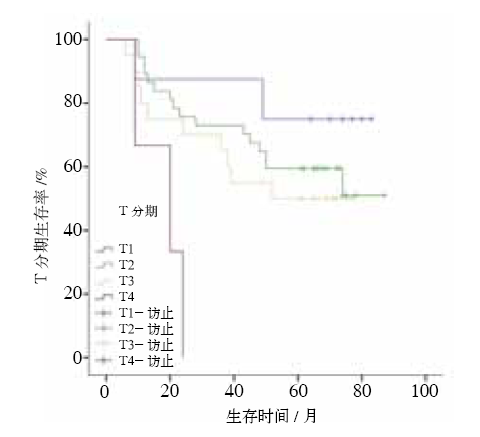
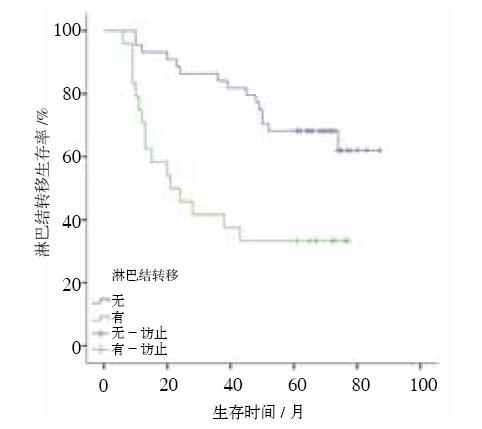
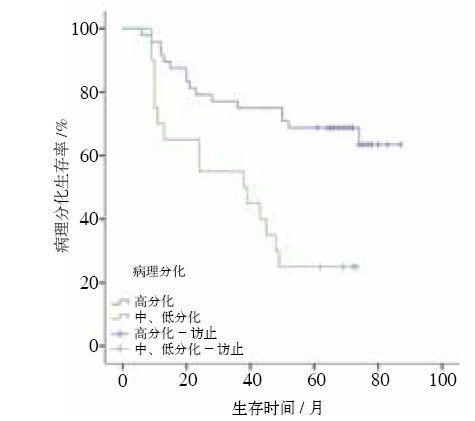
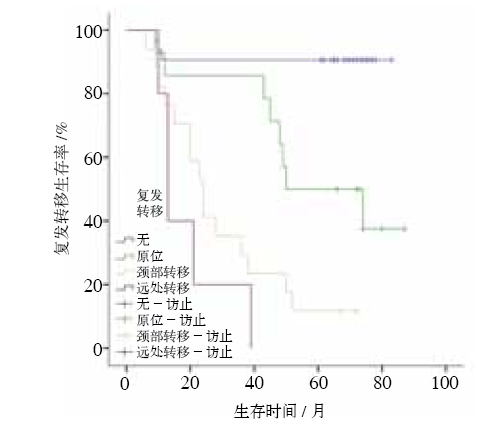
目的 分析口腔鳞状细胞癌(OSCC)患者的总体生存率,以及影响生存率的临床病理因素。方法 采集对首次接受根治性外科手术治疗的78例OSCC患者的临床病理及随访资料进行回顾性分析。对计数、计量资料进行描述性分析;采用Kaplan-Meier法绘制生存曲线;采用COX比例风险回归模型进行单因素和多因素分析,分析患者的生存率及预后相关影响因素。结果 最终纳入生存分析的患者共计68例,中位随访时间为63(6~87)个月,5年总体存活率为55.9%,随访期间因OSCC死亡患者的中位生存时间为20.5(6~52)个月。单因素分析表明,临床分期、原发灶大小、淋巴结转移、病理分化及复发转移是影响生存时间的暴露因素(P<0.05);多因素分析表明,病理分化、复发转移是影响生存时间的独立危险因素(P<0.05)。78例OSCC患者中合并发生食道鳞状细胞癌(ESCC)者有4例(5.1%)。结论 根据肿瘤的临床分期(TNM分期)、原发灶大小、淋巴结转移、病理分化及复发转移可对患者的生存预后作出一定的预测,其中病理分化及复发转移是影响生存预后的独立危险因素。有吸烟饮酒史的OSCC患者应常规进行ESCC临床筛查。
中图分类号:
| [1] | Siegel RL, Miller KD, Jemal A . Cancer statistics, 2016[J]. CA Cancer J Clin, 2016,66(1):7-30. |
| [2] | Götz C, Bissinger O, Nobis C , et al. ALDH1 as a prognostic marker for lymph node metastasis in OSCC[J]. Biomed Rep, 2018,9(4):284-290. |
| [3] | Sasahira T, Kirita T, Kuniyasu H . Update of mole-cular pathobiology in oral cancer: a review[J]. Int J Clin Oncol, 2014,19(3):431-436. |
| [4] | 曹雨庵, 郭伟 . 我国口腔鳞癌的治疗现状[J]. 实用肿瘤杂志, 2012,27(2):109-112. |
| Cao YA, Guo W . Treatment of oral squamous cell carcinoma in China[J]. J Pract Oncol, 2012,27(2):109-112. | |
| [5] | 陈新, 徐文华, 周健 , 等. 口腔鳞状细胞癌现状[J]. 口腔医学, 2017,37(5):462-465. |
| Chen X, Xu WH, Zhou J , et al. Current situation of oral squamous cell carcinoma[J]. Stomatology, 2017,37(5):462-465. | |
| [6] | Chen W, Zheng R, Zuo T , et al. National cancer incidence and mortality in China, 2012[J]. Chin J Cancer Res, 2016,28(1):1-11. |
| [7] | 王倩, 侯大为 . 口腔鳞状细胞癌发病及转移机制研究进展[J]. 口腔医学研究, 2018,34(11):1164-1167. |
| Wang Q, Hou DW . Research progress in pathogenesis of oral squamous cell carcinoma[J]. J Oral Sci Res, 2018,34(11):1164-1167. | |
| [8] | 贺智凤, 蒲玉梅, 胡勤刚 . 口腔鳞状细胞癌切缘状态评估及其影响因素分析[J]. 中华口腔医学杂志, 2017,52(7):445-449. |
| He ZF, Pu YM, Hu QG . Evaluation and influencing factors of surgical margin status of oral squamous cell carcinoma[J]. Chin J Stomatol, 2017,52(7):445-449. | |
| [9] | St John MA . Inflammatory mediators drive metastasis and drug resistance in head and neck squamous cell carcinoma[J]. Laryngoscope, 2015,125(Suppl 3):S1-S11. |
| [10] | Alves AM, Diel LF, Lamers ML . Macrophages and prognosis of oral squamous cell carcinoma: a syste-matic review[J]. J Oral Pathol Med, 2018,47(5):460-467. |
| [11] | de la Oliva J, Larque AB, Marti C , et al. Oral pre-malignant lesions of smokers and non-smokers show similar carcinogenic pathways and outcomes. A clin-icopathological and molecular comparative analysis[J]. J Oral Pathol Med, 2019. DOI: 10.1111/jop.12864. |
| [12] | Kumar B, Cordell KG, Lee JS , et al. EGFR, p16, HPV Titer, Bcl-xL and p53, sex, and smoking as indicators of response to therapy and survival in oropharyngeal cancer[J]. J Clin Oncol, 2008,26(19):3128-3137. |
| [13] | Rivera C . Essentials of oral cancer[J]. Int J Clin Exp Pathol, 2015,8(9):11884-11894. |
| [14] | Wolfer S, Elstner S, Schultze-Mosgau S . Degree of keratinization is an independent prognostic factor in oral squamous cell carcinoma[J]. J Oral Maxillofac Surg, 2018,76(2):444-454. |
| [15] | Chen F, Lin LS, Liu FQ , et al. Three prognostic in-dexes as predictors of response to adjuvant chemora-diotherapy in patients with oral squamous cell carcinoma after radical surgery: a large-scale prospective study[J]. Head Neck, 2019,41(2):301-308. |
| [16] | Weckx A, Riekert M, Grandoch A , et al. Time to re- currence and patient survival in recurrent oral squa-mous cell carcinoma[J]. Oral Oncol, 2019,94:8-13. |
| [17] | 张华, 杨蓉, 叶贝贝 , 等. 389例口腔鳞状细胞癌预后影响因素分析[J]. 天津医科大学学报, 2018,24(4):315-322. |
| Zhang H, Yang R, Ye BB , et al. Analysis of prognostic factors for 389 patients with oral squamous cell car-cinoma[J]. J Tianjin Med Univ, 2018,24(4):315-322. | |
| [18] | Colares N, Souza Rodrigues DF, Freitas MO , et al. Smoking history decreases survival in patients with squamous cell carcinoma of the mouth: a retros-pective study with 15 years of follow-up[J]. Asian Pac J Cancer Prev, 2019,20(6):1781-1787. |
| [19] | Montero PH, Yu CH, Palmer FL , et al. Nomograms for preoperative prediction of prognosis in patients with oral cavity squamous cell carcinoma[J]. Cancer, 2014,120(2):214-221. |
| [20] | Dissanayaka WL, Pitiyage G, Kumarasiri PV , et al. Clinical and histopathologic parameters in survival of oral squamous cell carcinoma[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2012,113(4):518-525. |
| [21] | Asio J, Kamulegeya A, Banura C . Survival and asso-ciated factors among patients with oral squamous cell carcinoma (OSCC) in Mulago hospital, Kam-pala, Uganda[J]. Cancers Head Neck, 2018,3:9. |
| [22] | Taghavi N, Yazdi I . Prognostic factors of survival rate in oral squamous cell carcinoma: clinical, histo-logic, genetic and molecular concepts[J]. Arch Iran Med, 2015,18(5):314-319. |
| [23] | Grimm M . Prognostic value of clinicopathological parameters and outcome in 484 patients with oral squamous cell carcinoma: microvascular invasion (V+) is an independent prognostic factor for OSCC[J]. Clin Transl Oncol, 2012,14(11):870-880. |
| [24] | Sandu K, Nisa L, Monnier P , et al. Clinicobiological progression and prognosis of oral squamous cell carcinoma in relation to the tumor invasive front: impact on prognosis[J]. Acta Otolaryngol, 2014,134(4):416-424. |
| [25] | Kane SV, Gupta M, Kakade AC , et al. Depth of in-vasion is the most significant histological predictor of subclinical cervical lymph node metastasis in early squamous carcinomas of the oral cavity[J]. Eur J Surg Oncol, 2006,32(7):795-803. |
| [26] | Mupparapu M, Shanti RM . Evaluation and staging of oral cancer[J]. Dent Clin North Am, 2018,62(1):47-58. |
| [27] | Kreppel M, Eich HT, Kübler A , et al. Prognostic value of the sixth edition of the UICC’s TNM classi-fication and stage grouping for oral cancer[J]. J Surg Oncol, 2010,102(5):443-449. |
| [28] | Huang TH, Li KY, Choi WS . Lymph node ratio as prognostic variable in oral squamous cell carcinomas: systematic review and meta-analysis[J]. Oral Oncol, 2019,89:133-143. |
| [29] | Yamagata K, Fukuzawa S, Kanno N , et al. Is lymph node ratio a prognostic factor for patients with oral squamous cell carcinoma[J]. J Oral Maxillofac Surg, 2019,77(7):1510-1519. |
| [30] | Ding D, Stokes W, Eguchi M , et al. Association be-tween lymph node ratio and recurrence and survival outcomes in patients with oral cavity cancer[J]. JAMA Otolaryngol Head Neck Surg, 2019,145(1):53-61. |
| [31] | Cuevas Gonzalez JC, Gaitan Cepeda LA, Borges Yanez SA , et al. p53 and p16 in oral epithelial dy-splasia and oral squamous cell carcinoma: a study of 208 cases[J]. Indian J Pathol Microbiol, 2016,59(2):153-158. |
| [32] | Zhuang ZH, Xie N, Hu J , et al. Interplay between ΔNp63 and miR-138-5p regulates growth, metastasis and stemness of oral squamous cell carcinoma[J]. Oncotarget, 2017,8(13):21954-21973. |
| [33] | Safadi RA, Abdullah NI, Alaaraj RF , et al. Clinical and histopathologic prognostic implications of the expression of cytokeratins 8, 10, 13, 14, 16, 18 and 19 in oral and oropharyngeal squamous cell carcinoma[J]. Arch Oral Biol, 2019,99:1-8. |
| [34] | Wang S, Sun M, Gu CW , et al. Expression of CD163, interleukin-10, and interferon-gamma in oral squa-mous cell carcinoma: mutual relationships and pro-gnostic implications[J]. Eur J Oral Sci, 2014,122(3):202-209. |
| [35] | Wang J, Jin X, Liu J , et al. The prognostic value of B7-H6 protein expression in human oral squamous cell carcinoma[J]. J Oral Pathol Med, 2017,46(9):766-772. |
| [36] | 黄江峰, 王靖雯, 何保昌 , 等. 口腔鳞状细胞癌患者生存影响因素研究[J]. 中华预防医学杂志, 2016,50(10):880-886. |
| Huang JF, Wang JW, He BC , et al. Study of survival factors of oral squamous cell carcinoma[J]. Chin J Prev Med, 2016,50(10):880-886. | |
| [37] | Wang B, Zhang S, Yue K , et al. The recurrence and survival of oral squamous cell carcinoma: a report of 275 cases[J]. Chin J Cancer, 2013,32(11):614-618. |
| [38] | Ghantous Y, Bahouth Z , Abu El-naaj I. Clinical and genetic signatures of local recurrence in oral squa-mous cell carcinoma[J]. Arch Oral Biol, 2018,95:141-148. |
| [39] | Aires FT, Lin CS, Matos LL , et al. Risk factors for distant metastasis in patients with oral cavity squa-mous cell carcinoma undergoing surgical treatment[J]. ORL J Otorhinolaryngol Relat Spec, 2017,79(6):347-355. |
| [40] | Jeon JH, Kim MG, Park JY , et al. Analysis of the outcome of young age tongue squamous cell carc-inoma[J]. Maxillofac Plast Reconstr Surg, 2017,39(1):41. |
| [41] | Luksic I, Suton P, Manojlovic S , et al. Significance of myofibroblast appearance in squamous cell car-cinoma of the oral cavity on the occurrence of occult regional metastases, distant metastases, and survival[J]. Int J Oral Maxillofac Surg, 2015,44(9):1075-1080. |
| [42] | Son HJ, Roh JL, Cho KJ , et al. Nodal factors predic-tive of recurrence and survival in patients with oral cavity squamous cell carcinoma[J]. Clin Otolaryngol, 2018,43(2):470-476. |
| [43] | Noble AR, Greskovich JF, Han J , et al. Risk factors associated with disease recurrence in patients with stage Ⅲ/Ⅳ squamous cell carcinoma of the oral cavity treated with surgery and postoperative radio-therapy[J]. Anticancer Res, 2016,36(2):785-792. |
| [44] | Brandwein-Gensler M, Wei S . Envisioning the next WHO head and neck classification[J]. Head Neck Pathol, 2014,8(1):1-15. |
| [45] | Meng F, Li RF, Ma LY , et al. Porphyromonas gin-givalis promotes the motility of esophageal squa-mous cell carcinoma by activating NF-κB signaling pathway[J]. Microbes Infect, 2019,21(7):296-304. |
| [46] | Smyth EC, Lagergren J, Fitzgerald RC , et al. Oeso-phageal cancer[J]. Nat Rev Dis Primers, 2017,3:17048. |
| [47] | Olsen I, Yilmaz Ö . Possible role of Porphyromonas gingivalis in orodigestive cancers[J]. J Oral Micro-biol, 2019,11(1):1563410. |
| [48] | Ha NH, Woo BH, Kim DJ , et al. Prolonged and re-petitive exposure to Porphyromonas gingivalis in-creases aggressiveness of oral cancer cells by promo-ting acquisition of cancer stem cell properties[J]. Tumor Biol, 2015,36(12):9947-9960. |
| [49] | Matsui T, Okada T, Kawada K , et al. Detection of second primary malignancies of the esophagus and hypophraynx in oral squamous cell carcinoma pa-tients[J]. Laryngoscope Investig Otolaryngol, 2018,3(4):263-267. |
| [1] | 周金阔,张晋弘,史晓晶,刘广顺,姜磊,刘倩峰. 长链非编码RNA小核仁RNA宿主基因22调控微小RNA-27b-3p对口腔鳞状细胞癌细胞增殖、侵袭和迁移的影响[J]. 国际口腔医学杂志, 2024, 51(1): 52-59. |
| [2] | 李立恒,王蕊,王晓明,张智轶,张璇,安峰,王芹,张凡. 环状RNA hsa_circ_0085576调控微小RNA-498/B细胞特异性莫洛尼鼠白血病病毒整合位点1轴对口腔鳞状细胞癌细胞迁移和侵袭的影响[J]. 国际口腔医学杂志, 2024, 51(1): 60-67. |
| [3] | 吴佳敏,夏斌,杨禾丰,许彪. 癌相关成纤维细胞在口腔鳞状细胞癌微环境中作用的研究进展[J]. 国际口腔医学杂志, 2023, 50(6): 711-717. |
| [4] | 柳江龙, 买买提吐逊·吐尔地. 超声造影在口腔鳞状细胞癌颈部转移性淋巴结诊断中的研究进展[J]. 国际口腔医学杂志, 2023, 50(5): 514-520. |
| [5] | 盛南宁,王珏,南欣荣. 性别决定基因盒9在口腔鳞状细胞癌作用机制和治疗中的研究进展[J]. 国际口腔医学杂志, 2023, 50(3): 314-320. |
| [6] | 王太萍,石兴莲,李喆臻,刘梅,姜健红. 口腔癌患者心理因素及干预现状分析[J]. 国际口腔医学杂志, 2023, 50(2): 203-209. |
| [7] | 李潭,梁新华. 盘状蛋白结构域受体1在调控恶性肿瘤进展和治疗中的作用[J]. 国际口腔医学杂志, 2023, 50(2): 230-236. |
| [8] | 尹茂运,张祎,胡敏. 正畸拔牙矫治对上气道影响的研究进展[J]. 国际口腔医学杂志, 2022, 49(5): 607-613. |
| [9] | 赵卓平,辛鹏飞,高阳,张彩凤,张宽收,刘青梅. 光热治疗在口腔鳞状细胞癌治疗中的研究进展[J]. 国际口腔医学杂志, 2022, 49(4): 462-470. |
| [10] | 江涵,神应强,陈谦明. 毒蕈碱受体通过Yes相关蛋白信号对口腔鳞状细胞癌生物学行为的实验研究[J]. 国际口腔医学杂志, 2022, 49(2): 138-143. |
| [11] | 吴兴胜,黄迪,石连水. 上颌窦过度气化及其影响因素的研究进展[J]. 国际口腔医学杂志, 2022, 49(2): 204-211. |
| [12] | 白皓亮,杨禾,赵蕾. 牙周病风险评估及预后判断工具的研究进展[J]. 国际口腔医学杂志, 2021, 48(6): 696-702. |
| [13] | 蒋宇磊,夏斌,饶南荃,杨禾丰,许彪. 外泌体在口腔鳞状细胞癌恶性进展及诊疗应用的研究[J]. 国际口腔医学杂志, 2021, 48(6): 711-717. |
| [14] | 马平川,李春洁,李龙江. 唾液腺导管癌的诊疗研究进展[J]. 国际口腔医学杂志, 2021, 48(4): 459-467. |
| [15] | 甘建国,高攀,王晓毅. 循环肿瘤细胞与口腔鳞状细胞癌相关性的研究进展[J]. 国际口腔医学杂志, 2021, 48(2): 205-212. |
|