国际口腔医学杂志 ›› 2020, Vol. 47 ›› Issue (5): 547-556.doi: 10.7518/gjkq.2020084
卫彬彬1( ),胡慧维1,刘玉娟1,孙哲2,衣玉丽1()
),胡慧维1,刘玉娟1,孙哲2,衣玉丽1()
Wei Binbin1(),Hu Huiwei1,Liu Yujuan1,Sun Zhe2,Yi Yuli1()
摘要:
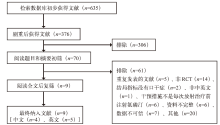
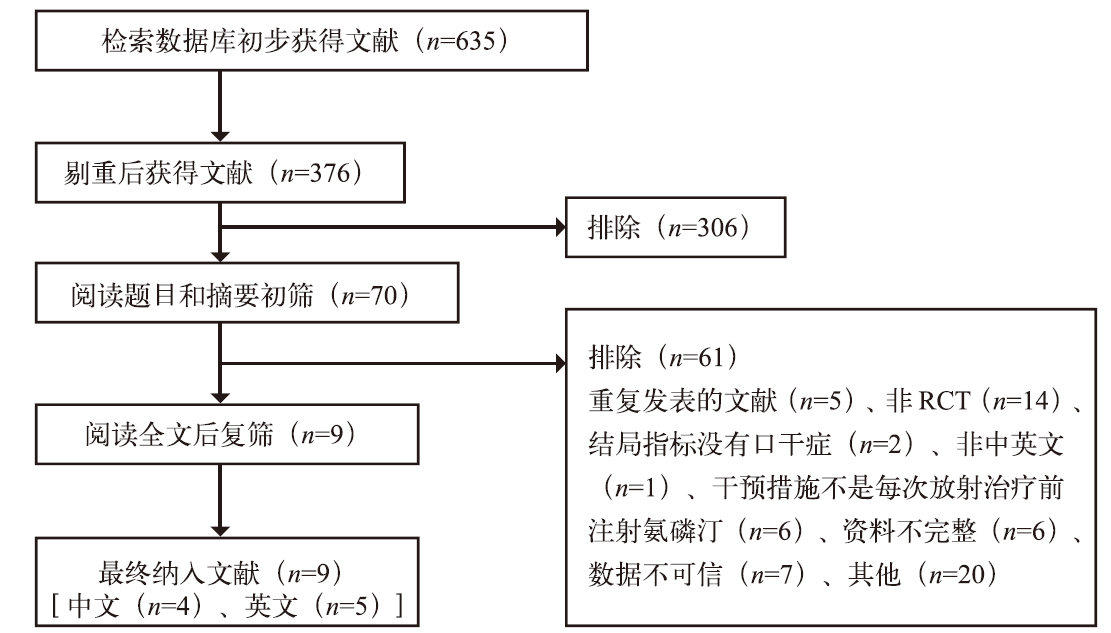
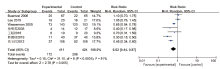
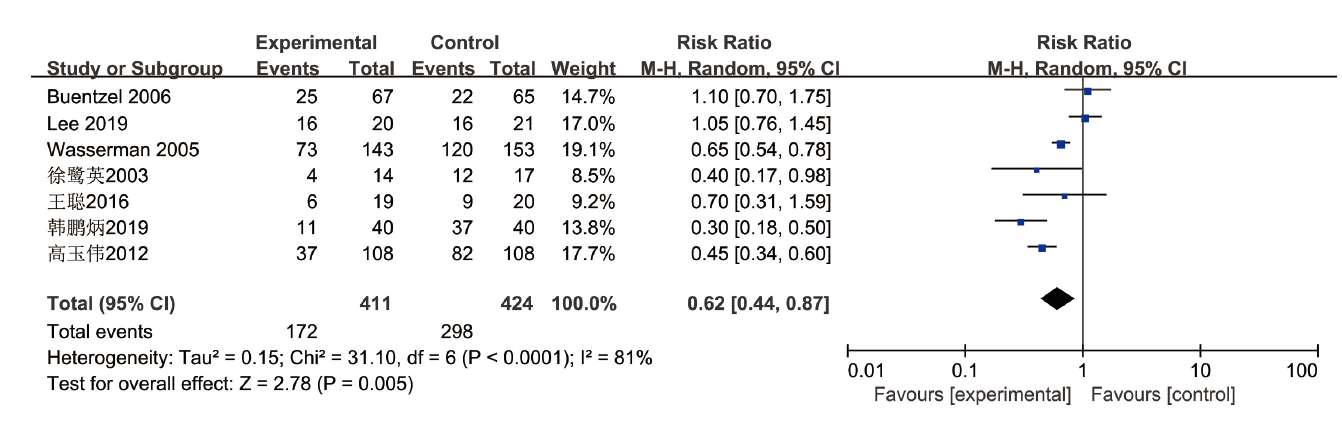
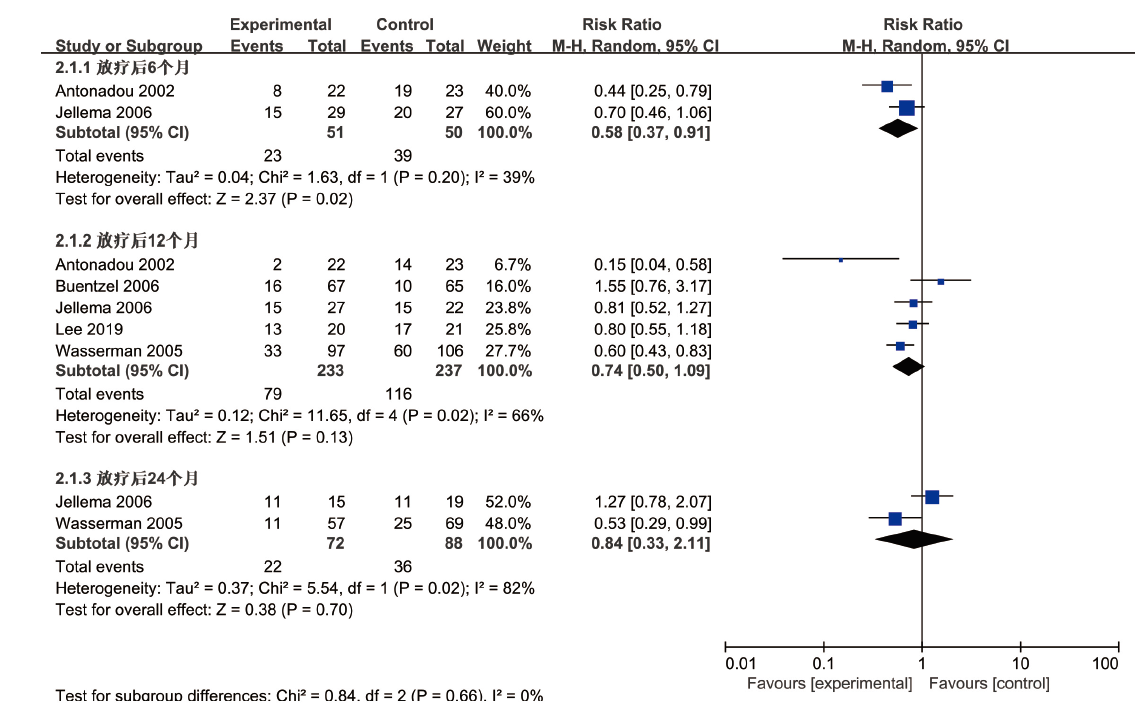
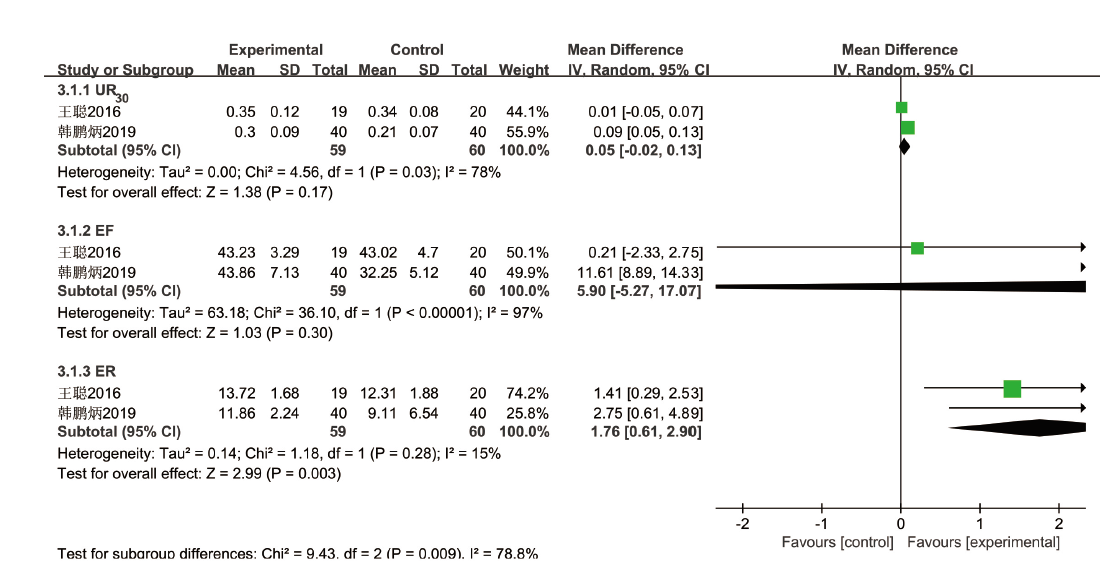
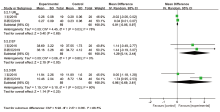
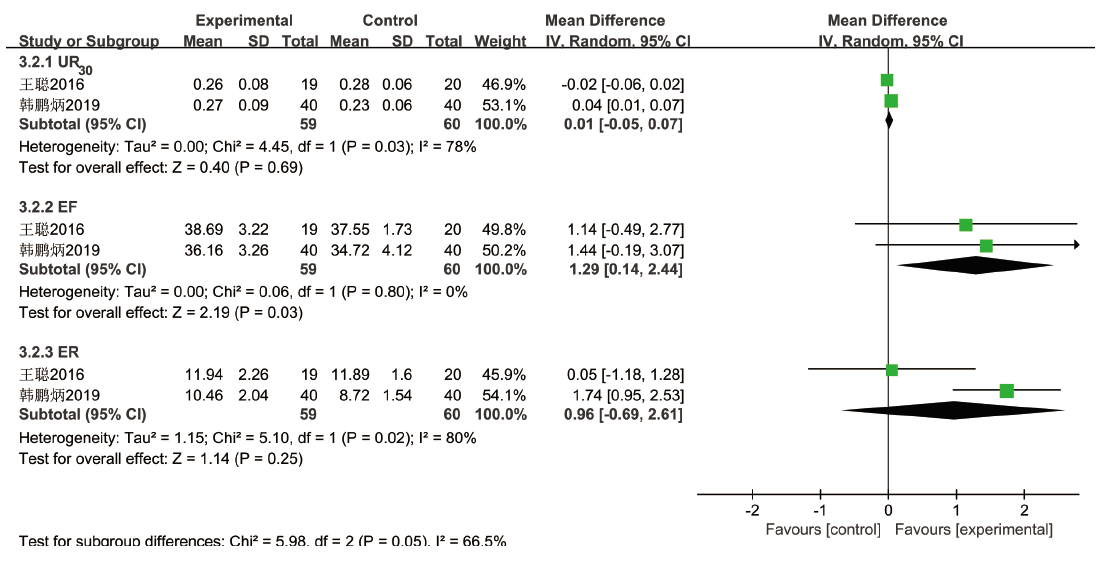
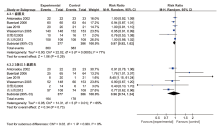
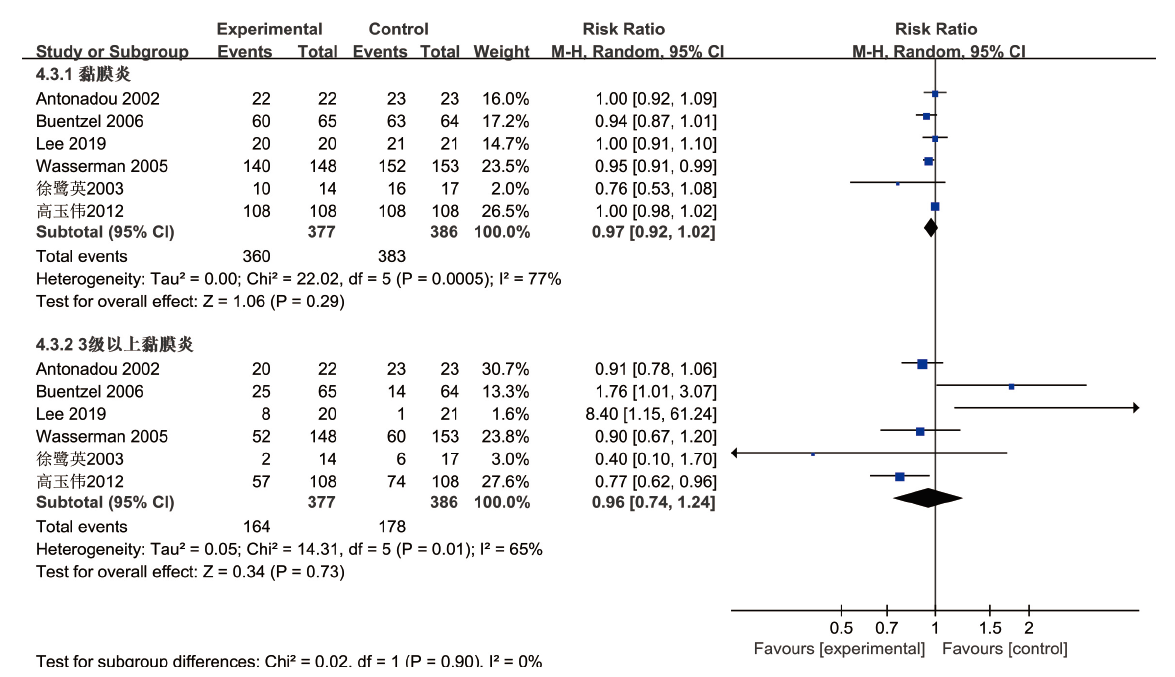
目的 评价放射治疗前使用氨磷汀对头颈部癌症患者口腔干燥等不良反应的干预效果。方法 检索中国知网(CNKI)、万方数据知识服务平台、中国生物医学文献数据库(CBMdisc)、维普中文科技期刊数据库(VIP)、PubMed、Cochrane Library、EMbase、Medline,从建库至2019年7月的相关中、英文文献,所检文献由2人按照纳入、排除标准进行筛选和质量评价,应用RevMan5.3软件进行Meta分析,并以GRADE证据分级系统对结局指标的证据质量进行评价。结果 最终纳入9篇随机对照试验(RCT),共948例患者。Meta分析结果显示,与对照组相比:氨磷汀减少了患者急性期[RR=0.62,95% CI(0.44,0.87),P=0.005]、放射治疗结束后6个月[RR=0.58,95% CI(0.37,0.91),P=0.02]2级以上口干,差异有统计学意义;在放射治疗结束后腺体功能指标、放射治疗结束12个月之后的晚期口干、急性黏膜炎、疾病控制、总体生存方面,差异无统计学意义(P>0.05);在不良反应恶心呕吐、低血压、过敏反应方面,不利于氨磷汀,差异有统计学意义(P<0.05)。GRADE证据质量评价结果显示,2级以上急性口干、恶心呕吐、过敏反应、局部区域控制、总体生存5个结局指标为中等质量证据,2级以上晚期口干、急性黏膜炎、低血压为低质量证据,而腺体功能指标为极低质量证据。结论 放射治疗前应用氨磷汀可减少头颈部癌症患者放射治疗急性期和放射治疗结束后6个月内的中重度口干发生,但对放射治疗后腺体功能、12个月之后的晚期口干和急性黏膜炎、肿瘤治疗效果没有积极影响,且其不良反应值得关注,还需更多大样本、高质量的研究来验证本结论。
中图分类号:
| [1] |
Siddiqui F, Movsas B. Management of radiation to-xicity in head and neck cancers[J]. Semin Radiat Oncol, 2017,27(4):340-349.
doi: 10.1016/j.semradonc.2017.04.008 pmid: 28865517 |
| [2] |
Riley P, Glenny AM, Hua F, et al. Pharmacological interventions for preventing dry mouth and salivary gland dysfunction following radiotherapy[J]. Cochrane Database Syst Rev, 2017, 7: CD012744.
doi: 10.1002/14651858.CD013684 pmid: 32691879 |
| [3] |
Strojan P, Hutcheson KA, Eisbruch A, et al. Treat-ment of late sequelae after radiotherapy for head and neck cancer[J]. Cancer Treat Rev, 2017,59:79-92.
pmid: 28759822 |
| [4] |
Vissink A, van Luijk P, Langendijk JA, et al. Current ideas to reduce or salvage radiation damage to sa-livary glands[J]. Oral Dis, 2015,21(1):e1-e10.
doi: 10.1111/odi.12222 pmid: 24581290 |
| [5] |
de Castro G Jr, Federico MH. Evaluation, prevention and management of radiotherapy-induced xerostomia in head and neck cancer patients[J]. Curr Opin Oncol, 2006,18(3):266-270.
doi: 10.1097/01.cco.0000219256.37843.83 pmid: 16552239 |
| [6] |
Jensen SB, Pedersen AM, Vissink A, et al. A syste-matic review of salivary gland hypofunction and xerostomia induced by cancer therapies: manage-ment strategies and economic impact[J]. Support Care Cancer, 2010,18(8):1061-1079.
doi: 10.1007/s00520-010-0837-6 |
| [7] | 龙小庆, 王继生, 贾霖, 等. 三乙醇胺防治放射性皮炎有效性的Meta分析及GRADE证据质量评价[J]. 中国药房, 2019,30(2):258-263. |
| Long XQ, Wang JS, Jia L , et al. Meta-analysis of the effectiveness of trolamine for preventing and treating radiation dermatitis and quality evaluation of GRADE evidence[J]. China Pharm, 2019,30(2):258-263. | |
| [8] |
Antonadou D, Pepelassi M, Synodinou M, et al. Pro-phylactic use of amifostine to prevent radiochemo-therapy-induced mucositis and xerostomia in head-and-neck cancer[J]. Int J Radiat Oncol Biol Phys, 2002,52(3):739-747.
doi: 10.1016/s0360-3016(01)02683-9 pmid: 11849797 |
| [9] | 徐鹭英, 潘建基, 杨凌, 等. 氨磷汀减少鼻咽癌放射治疗中唾液腺损伤的临床研究[J]. 福建医药杂志, 2003,25(4):61-62. |
| Xu LY, Pan JJ, Yang L , et al. Clinical study of ami-fostine in reducing salivary gland injury in radio-therapy of nasopharyngeal carcinoma[J]. Fujian Med J, 2003,25(4):61-62. | |
| [10] |
Jellema AP, Slotman BJ, Muller MJ, et al. Radiothe-rapy alone, versus radiotherapy with amifostine 3 times weekly, versus radiotherapy with amifostine 5 times weekly: a prospective randomized study in squamous cell head and neck cancer[J]. Cancer, 2006,107(3):544-553.
pmid: 16804929 |
| [11] |
Buentzel J, Micke O, Adamietz IA, et al. Intravenous amifostine during chemoradiotherapy for head-and-neck cancer: a randomized placebo-controlled phase Ⅲ study[J]. Int J Radiat Oncol Biol Phys, 2006,64(3):684-691.
pmid: 16243440 |
| [12] | 高玉伟, 尹立杰, 丁田贵, 等. 氨磷汀减轻头颈部恶性肿瘤放疗损伤的临床观察[J]. 中国肿瘤临床与康复, 2012,19(6):499-501. |
| Gao YW, Yin LJ, Ding TG , et al. Clinical treatment of amifostine reduces radiation injury on head and neck cancer[J]. Chin J Clin Oncol Rehabilitation, 2012,19(6):499-501. | |
| [13] |
Wasserman TH, Brizel DM, Henke M, et al. Influence of intravenous amifostine on xerostomia, tumor con-trol, and survival after radiotherapy for head-and-neck cancer: 2-year follow-up of a prospective, randomized, phase Ⅲ trial[J]. Int J Radiat Oncol Biol Phys, 2005,63(4):985-990.
doi: 10.1016/j.ijrobp.2005.07.966 pmid: 16253773 |
| [14] |
Lee MG, Freeman AR, Roos DE, et al. Randomized double-blind trial of amifostine versus placebo for radiation-induced xerostomia in patients with head and neck cancer[J]. J Med Imaging Radiat Oncol, 2019,63(1):142-150.
pmid: 30461207 |
| [15] | 韩鹏炳, 冀雪娟, 高力英, 等. 氨磷汀对鼻咽癌放射治疗中唾液腺功能的保护作用[J]. 中国辐射卫生, 2019,28(1):98-101. |
| Han PB, Ji XJ, Gao LY , et al. Protective effect of amifostine on salivary gland function in radiotherapy of nasopharyngeal carcinoma[J]. Chin J Radiol Heal, 2019,28(1):98-101. | |
| [16] | 王聪. 131I治疗DTC时维生素C和氨磷汀对唾液腺保护作用研究 [D]. 太原: 山西医科大学, 2016. |
| Wang C . A comparative study of the protective effect of vitamin C and amifostine to salivary gland function of differentiated thyroid cancer after application 131I [D]. Taiyuan: Shanxi Medical University, 2016. | |
| [17] |
Cohen EE, LaMonte SJ, Erb NL, et al. American cancer society head and neck cancer survivorship care guideline[J]. CA Cancer J Clin, 2016,66(3):203-239.
pmid: 27002678 |
| [18] |
Likhterov I, Ru M, Ganz C, et al. Objective and sub-jective hyposalivation after treatment for head and neck cancer: long-term outcomes[J]. Laryngoscope, 2018,128(12):2732-2739.
doi: 10.1002/lary.27224 pmid: 30325025 |
| [19] |
Schuchter LM, Hensley ML, Meropol NJ, et al. 2002 update of recommendations for the use of chemothe-rapy and radiotherapy protectants: clinical practice guidelines of the American Society of Clinical Onco-logy[J]. J Clin Oncol, 2002,20(12):2895-2903.
doi: 10.1200/JCO.2002.04.178 pmid: 12065567 |
| [20] |
Ma SJ, Rivers CI, Serra LM, et al. Long-term out-comes of interventions for radiation-induced xeros-tomia: a review[J]. World J Clin Oncol, 2019,10(1):1-13.
doi: 10.5306/wjco.v10.i1.1 pmid: 30627521 |
| [21] |
Sasse AD, Clark LG, Sasse EC, et al. Amifostine reduces side effects and improves complete response rate during radiotherapy: results of a meta-analysis[J]. Int J Radiat Oncol Biol Phys, 2006,64(3):784-791.
pmid: 16198504 |
| [22] |
Gu JD, Zhu SW, Li XB, et al. Effect of amifostine in head and neck cancer patients treated with radiothe-rapy: a systematic review and meta-analysis based on randomized controlled trials[J]. PLoS One, 2014,9(5):e95968.
pmid: 24788761 |
| [23] |
Riley P, Glenny AM, Worthington HV, et al. Inter-ventions for preventing oral mucositis in patients with cancer receiving treatment: cytokines and growth factors[J]. Cochrane Database Syst Rev, 2017, 11: CD011990.
pmid: 30484282 |
| [24] | 朱秋霞, 张振勇, 吴荣. 阿米福汀在头颈肿瘤放疗中的应用进展[J]. 医学综述, 2014,20(4):662-665. |
| Zhu QX, Zhang ZY, Wu R . Research progress in ap-plication of amifostine in radiotherapy of head and neck tumor[J]. Med Recapitul, 2014,20(4):662-665. |
| [1] | 和子慕, 李风兰. 数字化口腔定位支架在头颈部肿瘤放射治疗中的应用现状[J]. 国际口腔医学杂志, 2024, 51(1): 28-35. |
| [2] | 杨明燕,张帆,赵蕾. 口腔菌群变化影响放射治疗和化学治疗相关性口腔黏膜炎病程的研究进展[J]. 国际口腔医学杂志, 2023, 50(1): 43-51. |
| [3] | 陈小利,张帆,刘程程. 光生物调节在放射治疗后口腔并发症防治中的应用进展[J]. 国际口腔医学杂志, 2022, 49(6): 707-716. |
| [4] | 李洪芳,陈中,张素欣. 免疫检查点抑制剂联合放射治疗在头颈部鳞状细胞癌治疗中的研究进展[J]. 国际口腔医学杂志, 2022, 49(5): 614-620. |
| [5] | 陈东,杨征,蒋丽. 放射性口腔干燥症的评估与临床管理的研究进展[J]. 国际口腔医学杂志, 2019, 46(6): 711-717. |
| [6] | 吕丹妮,李容林,杨光伟,李春阳. 放射治疗和化学治疗诱发性口腔黏膜炎的防治[J]. 国际口腔医学杂志, 2015, 42(2): 177-180. |
| [7] | 陈琦 吴芸. 肿痛安治疗癌症放射治疗后颞下颌关节疼痛的疗效评价[J]. 国际口腔医学杂志, 2015, 42(1): 24-27. |
| [8] | 王亚敏综述 宋光保审校. 放射治疗对口腔种植的影响[J]. 国际口腔医学杂志, 2011, 38(2): 204-206. |
| [9] | 夏勇综述 农晓琳审校. 涎腺恶性肿瘤治疗方法的研究进展[J]. 国际口腔医学杂志, 2009, 36(1): 46-46~49. |
|